
Bladder cancer
Making treatment decisions
Bladder cancer treatment depends on the stage, grade and your own preferences. Learn about each approach, possible side effects, and how to make informed decisions with your specialist treatment team.


Last updated:
Sources and references What's on this page
- Superficial bladder cancer treatment
- Surgery (TURBT)
- Intravesical chemotherapy
- Intravesical immunotherapy (BCG)
- Key points about treating superficial bladder cancer
- Muscle-invasive bladder cancer treatment
- Surgery (cystectomy)
- Surgery to remove the bladder
- Systemic chemotherapy
- Immunotherapy (checkpoint inhibitors)
- Radiation therapy
- Trimodal therapy
- Key points about treating muscle-invasive bladder cancer
- Urinary diversion
- Urostomy
- Neobladder
- Continent urinary diversion

Sometimes it is difficult to decide on the type of treatment to have. You may feel that everything is happening too fast, or you might be anxious to get started.
Check with your specialist how soon treatment should begin, as it may not affect the success of the treatment to wait a while. Ask them to explain the options, and take as much time as you can before making a decision.
Know your options
Understanding the disease, the available treatments, possible side effects and any extra costs can help you weigh up the options and make a well informed decision. Check if the specialist is part of a multidisciplinary team and if the treatment centre is the most appropriate one for you – you may be able to have treatment closer to home, or it might be worth travelling to a centre that specialises in a particular treatment.
Record the details
When your doctor first says you have cancer, you may not remember everything you are told. Taking notes can help. If you would like to record the discussion, ask your doctor first. It is a good idea to have a family member or friend go with you to appointments to join in the discussion, write notes or simply listen.
Ask questions
If you are confused or want to check anything, it is important to ask your specialist questions. Try to prepare a list before appointments. If you have a lot of questions, you could talk to a cancer care coordinator or nurse.
Consider a second opinion
You may want to get a second opinion from another specialist to confirm or clarify your specialist’s recommendations or reassure you that you have explored all of your options. Specialists are used to people doing this. Your GP or specialist can refer you to another specialist and send your initial results to that person. You can get a second opinion even if you have started treatment or still want to be treated by your first doctor. You might decide you would prefer to be treated by the second specialist.
It's your decision
Adults have the right to accept or refuse any treatment that they are offered. For example, some people with advanced cancer choose treatment that has significant side effects even if it gives only a small benefit for a short period of time. Others decide to focus their treatment on quality of life. You may want to discuss your decision with the treatment team, GP, family and friends.
Should I join a clinical trial?
Your doctor or nurse may suggest you take part in a clinical trial. Doctors run clinical trials to test new or modified treatments and ways of diagnosing disease to see if they are better than current methods. For example, if you join a randomised trial for a new treatment, you will be chosen at random to receive either the best existing treatment or the modified new treatment. Over the years, trials have improved treatments and led to better outcomes for people diagnosed with cancer.
You may find it helpful to talk to your specialist, clinical trials nurse or GP, or to get a second opinion. If you decide to take part in a clinical trial, you can withdraw at any time. For more information, visit australiancancertrials.gov.au.
What to do before and after treatment
Talk with your doctors about what you can do to prepare for treatment and help your recovery. Your doctors may suggest that you:
Stop smoking
If you smoke, aim to quit before starting treatment. If you keep smoking, you may not respond as well to treatment and you may have more treatment-related side effects.For support, see your doctor or call Quitline 13 7848.
Begin or continue an exercise program
Exercise will help build up your strength for treatment and recovery. It can also help you deal with the side effects of treatment. Talk to your doctor, exercise physiologist or physiotherapist about the right type of exercise for you.
Improve your diet and avoid alcohol
Aim to eat a balanced diet with a variety of vegetables, fruit, wholegrains and protein. Eating well can improve your strength and you may respond better to treatment. Limiting how much you drink may also be advised, as alcohol can increase the risk of some types of cancer.
See a physiotherapist
They can teach you exercises to strengthen your pelvic floor muscles, which help control your bladder and bowel. It’s important to do these exercises after some types of treatment and if you have a neobladder.
Superficial bladder cancer treatment
If cancer cells are found only in the inner layers of the bladder, the cancer is called superficial or non-muscle-invasive bladder cancer (NMIBC). The main treatment for superficial bladder cancer is surgery to remove the cancer. This is often done during diagnosis. Surgery is commonly combined with chemotherapy or immunotherapy, which is delivered directly into the bladder (intravesical).
Surgery (TURBT)
Most people with superficial bladder cancer have an operation called transurethral resection of bladder tumour or TURBT. This procedure is usually done during diagnosis.
If the cancer has spread to the lamina propria or is high grade, you may need a second TURBT 2–6 weeks after the first procedure to make sure that all cancer cells are removed. If the cancer comes back after initial treatment, your surgeon may do another TURBT or suggest removing the bladder in an operation called a cystectomy.
Check-ups after surgery
Cancer can come back even after a TURBT has removed it from the bladder. You will need regular follow-up cystoscopies to find any new tumours in the bladder as early as possible. This approach is known as surveillance cystoscopy.
How often you need to have a cystoscopy will depend on the stage and grade of the cancer, and how long since it was diagnosed.
Intravesical chemotherapy
Chemotherapy uses drugs to kill or slow the growth of cancer cells. The aim is to destroy cancer cells while causing the least possible damage to healthy cells.
Chemotherapy drugs are usually injected into a vein or given as tablets. In intravesical chemotherapy, the drugs are put directly into the bladder using a catheter (a thin, flexible tube) inserted through the urethra.
Intravesical chemotherapy is used mainly for low-risk to medium-risk superficial bladder cancer. It helps prevent the cancer coming back (called a recurrence).
Each dose is called an instillation, and this is usually given in a day procedure in hospital.
People with a low risk of recurrence usually have one instillation straight after TURBT surgery. The chemotherapy solution is left in the bladder for 1–2 hours and then drained out through a catheter or by urinating after the catheter has been removed. You may be asked to change position every 15 minutes so the solution washes over the whole bladder.
People with a medium risk of recurrence may have instillations once a week for about 6 weeks. While you are having a course of intravesical chemotherapy, your doctor may advise you to use contraception.
Side effects of intravesical chemotherapy
Because intravesical chemotherapy puts the drugs directly into the bladder, it has fewer side effects than systemic chemotherapy (when the drugs spread through the whole body).
The main side effect of intravesical chemotherapy is inflammation of the bladder lining (called cystitis). Signs of cystitis include wanting to pass urine more often or having a burning feeling when urinating. Drinking plenty of fluids can help. If you develop a bladder infection, your doctor can prescribe antibiotics.
In some people, intravesical chemotherapy may cause a rash on the hands or feet. Tell your doctor if you notice any side effects while on intravesical chemotherapy.
Intravesical immunotherapy (BCG)
Immunotherapy is treatment that uses the body’s own natural defences (the immune system) to fight disease. Bacillus Calmette-Guérin (BCG) is a vaccine that was originally used to prevent tuberculosis. It can also stimulate a person’s immune system to stop or delay bladder cancer coming back or becoming invasive.
The most effective way to treat high-risk superficial bladder cancer is with a combination of BCG and TURBT. Some time after TURBT surgery, BCG will be given once a week for about 6 weeks. BCG is put directly into the bladder through a catheter.
You may be asked to change position every 15 minutes so the vaccine washes over the whole bladder. This is usually done as a day procedure in hospital, and each treatment session takes up to 2 hours.
The BCG vaccine contains live bacteria, which can harm healthy people, so your treatment team will tell you what safety measures to follow at home. Speak to your medical team if you have any questions.
BCG safety at home
Take care going to the toilet
For 6 hours after BCG treatment, sit on the toilet when urinating to avoid splashing. When finished, pour 2 cups of household bleach (or a sachet of sodium hypochlorite if provided by your treatment team) into the toilet bowl. Wait 15 minutes before flushing twice with the toilet lid closed. Wipe the seat with disinfectant. If clothing is splashed with urine, wash separately in bleach and warm water.
Drink fluids
To help clear the BCG from your body, drink plenty of liquids for 6-8 hours after treatment.
Handle incontinence pads carefully
If you use incontinence pads, for a few days after treatment take care when disposing of them. Pour bleach on the used pad, allow it to soak in, then place the pad in a plastic bag. Tie up the bag and put it in your rubbish bin. You may also be able to take the sealed bag back to the hospital or treatment centre for disposal in a biohazard bin.
Practice safe sex
For a week after each treatment, use barrier contraception (condoms) to protect your partner from any BCG that may be present in your body fluids and to prevent pregnancy.
Wash hands well
For a few days after each treatment, wash your hands extra well after going to the toilet. If your skin comes in contact with urine, wash or shower with soap and water.
Ongoing BCG treatment
For most people with high-risk superficial bladder cancer, the initial, 6-week course of BCG treatments is followed by more BCG. This is called maintenance BCG and it reduces the risk of the disease coming back or spreading.
Maintenance treatment can last for 1–3 years, but treatment sessions become much less frequent (e.g. one dose a month). Treatment schedules can vary so ask your doctor for further details and see the opposite page for safety measures to take at home.
Side effects of BCG
Common side effects of BCG include needing to urinate more often; burning or pain when urinating; blood in the urine; a mild fever; and tiredness. These side effects usually last a couple of days after each BCG treatment session.
Less often, the BCG may spread through the body and can affect any organ. If you develop flu-like symptoms, such as fever over 38°C that lasts longer than 72 hours, pain in your joints, a cough, a skin rash, tiredness, or yellow skin (jaundice), contact a nurse or doctor at your treatment centre immediately. A BCG infection can be treated with medicines.
Very rarely, BCG can cause infections in the lungs or other organs months or years after treatment. If you are diagnosed with an infection in the future, it is important to tell the doctor that you had BCG treatment.
Key points about treating superficial bladder cancer
Surgery
- Most people with superficial bladder cancer (also known as non-muscle-invasive bladder cancer or NMIBC) have a transurethral resection of bladder tumour (TURBT) operation.
- A TURBT is done during a rigid cystoscopy under general anaesthetic. It is often done during diagnosis.
- It is common to have treatments such as intravesical chemotherapy and intravesical immunotherapy after the surgery.
- TURBT can be repeated if the cancer returns.
Intravesical chemotherapy
- Intravesical chemotherapy is used for low-risk to medium-risk superficial bladder cancer.
- It places the drugs directly into the bladder through a catheter.
- Each treatment is called an instillation.
- The most common side effect is bladder inflammation (cystitis).
Intravesical immunotherapy
- Bacillus Calmette-Guérin (BCG) is a vaccine used to prevent tuberculosis. It is used for high-risk superficial bladder cancer.
- When used to treat superficial bladder cancer, it is put directly into the bladder through a catheter to encourage the body’s immune system to try to destroy the cancer.
- You will usually have BCG once a week for 6 weeks, followed by long-term maintenance therapy.
- You will need to take some safety precautions at home after BCG treatment.
- Side effects, such as urinary issues, a mild fever and tiredness, usually last a couple of days.
Muscle-invasive bladder cancer treatment
When bladder cancer has invaded the muscle layer (muscularis propria), the main treatment options are:
- surgery to remove the whole bladder (cystectomy), sometimes with chemotherapy given before surgery (neoadjuvant chemotherapy) or after surgery (adjuvant chemotherapy).
- bladder-conserving surgery (TURBT), followed by radiation therapy with or without chemotherapy. This is called trimodal therapy.
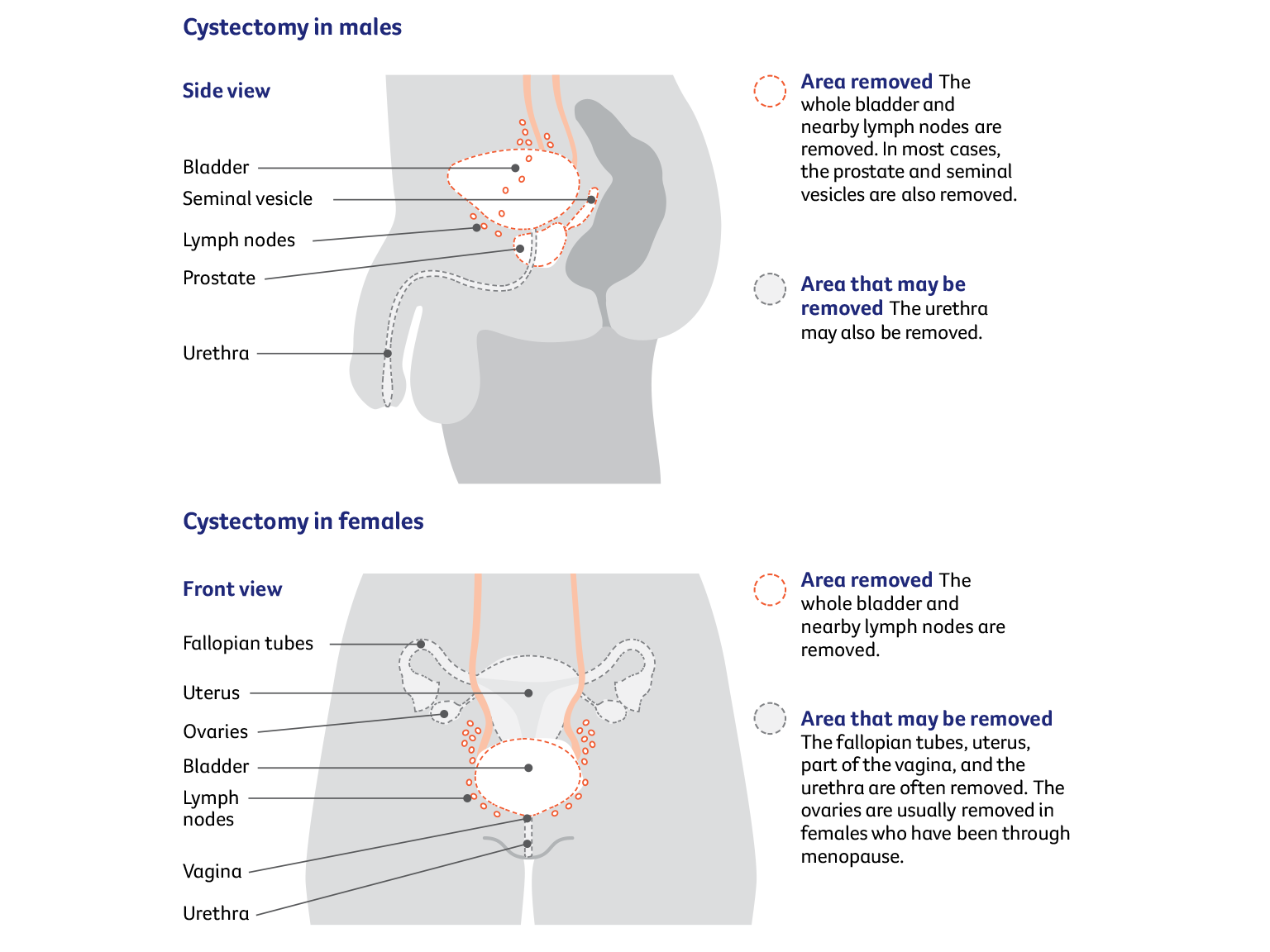
Surgery (cystectomy)
Some people with muscle-invasive disease have surgery to remove the bladder (cystectomy). This may also be recommended for high-risk superficial bladder cancer (also called non-muscle-invasive bladder cancer or NMIBC) that has not responded to BCG. The surgeon usually needs to remove the whole bladder and nearby lymph nodes. This is called a radical cystectomy.
How the surgery is done
Surgery to remove the bladder and create a urinary diversion is a complicated operation. Different surgical methods may be used to remove the bladder:
- Open surgery makes one long cut (incision) in the lower abdomen. A cut is usually made from below the belly button to the pubic area.
- Keyhole surgery, also known as minimally invasive or laparoscopic surgery, makes several smaller cuts in the abdomen. Instruments are inserted through the cuts, sometimes with help from a robotic system.
It is important to have this surgery in a specialised centre with a surgeon who does a lot of cystectomies. In general, having an experienced surgeon is more important than the type of surgery. Talk to your surgeon about the pros and cons of each surgical method, and check what you’ll have to pay. Unless you are treated as a public patient in a public hospital, you are likely to have lots of costs not covered by Medicare or your health fund.
What to expect after surgery
When you wake up after the operation, you will be in a recovery room near the operating theatre. Once you are fully conscious, you will be moved to intensive care or to the ward.
Tubes and drips – You may have an intravenous (IV) drip to give you fluid and medicine, and a tube in your abdomen to drain fluid from the operation area. These will be removed as you recover.
Pain and discomfort – After a major operation, it is common to feel some pain. You will be given pain medicine as a tablet (orally), through a drip (intravenously) or through a catheter inserted in the spaces in the spine (epidural) or along the wound (wound catheters). If you still have pain, let your doctor or nurse know and they may change your medicine.
Recovery time – You will probably be in hospital for 1–2 weeks, but it can take 6–8 weeks to fully recover from a cystectomy. The recovery time will depend on the type of surgery, your fitness and whether you have any complications.
Passing urine – Because a radical cystectomy removes the whole bladder, the surgeon needs to create a new way for your body to store and pass urine.
Surgery to remove the bladder
The most common operation for muscle-invasive bladder cancer is a radical cystectomy. The surgeon removes the whole bladder and nearby lymph nodes. Other organs may also be removed. After a radical cystectomy, a urinary diversion is needed so your body can store and pass urine.
Sexual activity and fertility after cystectomy
A cystectomy can affect sexual activity and fertility in many ways. You may find these changes upsetting and worry about how they’ll affect your relationships. Ask your treatment team for information about ways to manage these changes. It may be helpful to talk about how you’re feeling with your partner, family members or a counsellor.
Changes for males
Nerve damage to the penis
A cystectomy can often damage nerves to the penis, but the surgeon will try to prevent or minimise this. Nerve damage can make it difficult to get an erection. Options for improving erections include:
- oral medicines prescribed by a doctor that increase blood flow to the penis
- injections of medicine into the penis
- vacuum devices that use suction to draw blood into the penis and make it firm
- an implant called a penile prosthesis – under general anaesthetic, flexible rods or thin inflatable cylinders are inserted into the penis and a pump is placed in the scrotum; you can then turn on or squeeze the pump when you want an erection.
Orgasm changes
If the prostate and seminal vesicles are removed along with the bladder, you will not be able to ejaculate after a radical cystectomy. You can still feel the muscular spasms and pleasure of an orgasm even if you cannot ejaculate or get an erection, but it will be a dry orgasm because you no longer produce semen.
Fertility changes
If the prostate and seminal vesicles are removed, you will no longer produce semen. This means you won’t be able to have children naturally. If you might want to have children in the future, talk to your treatment team about whether you can store sperm at a fertility clinic before treatment. The sperm could then be used when you are ready to start a family.
Changes for females
Vaginal changes
Sometimes, the vagina may be shortened or narrowed during a cystectomy. Nerves that help keep the vagina moist can also be affected, making the vagina dry. These changes can make penetrative sex difficult or uncomfortable at first. Ways to manage these changes include:
- using a hormone cream (available on prescription) or vaginal moisturiser (available at pharmacies) to keep your vagina moist
- asking a physiotherapist how to use vaginal dilators to help stretch the vagina – vaginal dilators are plastic or rubber tube-shaped devices that come in different sizes
- when you feel ready, trying to have sex regularly and gently to stretch the vagina
- using a water-based or silicone-based lubricant (available from pharmacies and supermarkets) to make sex more comfortable.
Arousal changes
A cystectomy can damage the nerves in the vagina or reduce the blood supply to the clitoris, which can affect how you become aroused and your ability to orgasm. Talk to your surgeon or nurse about ways to minimise potential side effects. You can also try exploring other areas of your body that feel pleasurable when touched, such as the breasts, inner thighs, feet or buttocks.
Menopause and fertility
Sometimes, the uterus and other reproductive organs are removed during a radical cystectomy. This will cause menopause if you have not already been through it. Your periods will stop, you will no longer be able to become pregnant, and you may have menopausal symptoms such as hot flushes and vaginal dryness. Talk to your doctors about ways to deal with symptoms of menopause.
Systemic chemotherapy
Chemotherapy uses drugs to kill or slow the growth of cancer cells. For muscle-invasive bladder cancer, drugs are injected into a vein (intravenously) and travel throughout the body. This type of chemotherapy is called systemic chemotherapy. It is different to the intravesical chemotherapy used for superficial bladder cancer, which is delivered directly into the bladder.
Systemic chemotherapy for muscle-invasive bladder cancer is used:
- before surgery (neoadjuvant chemotherapy) – to shrink the cancer and make it easier to remove; it can also lower the risk of the cancer coming back
- after surgery (adjuvant chemotherapy) – if there is a high risk of the cancer coming back.
How chemotherapy is given – Chemotherapy is commonly given as a period of treatment followed by a break. This is called a cycle. In most cases, you will have several cycles of chemotherapy over a few months. Usually, a combination of drugs works better than one drug alone.
Systemic chemotherapy can sometimes be combined with radiation therapy (chemoradiation) and TURBT as part of trimodal therapy. Systemic chemotherapy may also be used for bladder cancer that has spread to other parts of the body.
Side effects of systemic chemotherapy – These may include: fatigue; nausea and vomiting; constipation; mouth sores; taste changes; itchy skin; hair loss; ringing in the ears; and tingling or numbness of the fingers or toes. Side effects usually last for only a few weeks or months, although some can be permanent. Talk to your doctor about ways to reduce your risk or manage any side effects you develop.
During chemotherapy, you may be more prone to infections. If you develop a temperature over 38°C, contact your doctor or go immediately to the emergency department at your nearest hospital.
Immunotherapy (checkpoint inhibitors)
This type of drug treatment uses the body's own immune system to fight cancer. In muscle-invasive bladder cancer, immunotherapy drugs may be used with chemotherapy before surgery (neoadjuvant treatment) or after surgery (adjuvant treatment).
How immunotherapy is given – Immunotherapy is given in the same way as chemotherapy.
Side effects of immunotherapy – This treatment may trigger an immune response that leads to side effects anywhere in the body. Other side effects include fatigue, headaches and nausea and vomiting.
Radiation therapy
Radiation therapy, also called radiotherapy, uses a controlled dose of radiation to kill or damage cancer cells. The radiation is usually in the form of x-ray beams. Radiation therapy to treat bladder cancer may be used on its own, combined with chemotherapy (chemoradiation) or as part of trimodal therapy.
How radiation therapy is given – You will meet with the radiation oncology team to plan your treatment. It is common to have imaging scans to help locate the area to receive the radiation.
During treatment, you will lie on an examination table and a machine will direct the radiation towards your bladder. The treatment is painless.
Side effects of radiation therapy – Temporary side effects may include: needing to urinate more often and more urgently; a burning sensation when you urinate; fatigue; loss of appetite; diarrhoea; and soreness around the anus. Symptoms tend to build up during treatment and usually start improving a few weeks after treatment ends.
Less commonly, radiation therapy may permanently affect the bowel or bladder. Bowel motions may be more frequent and looser, and damage to the bladder lining (radiation cystitis) can cause blood in the urine.
Radiation therapy for males may cause poor erections and make ejaculation uncomfortable for some months after treatment. For females, radiation therapy can cause the vagina to become drier, narrower and shorter. It may also lead to premature menopause. If the therapy affects the lymph nodes, there may be an increased risk of lymphoedema (swelling in the legs caused by a build-up of lymph fluid).
Trimodal therapy
Instead of a cystectomy, you may have trimodal therapy as the main treatment for muscle-invasive bladder cancer. Trimodal therapy may be used if a person is unable to have surgery to remove the bladder or would prefer to keep their bladder. It is most suited for people whose bladder is working well and who have smaller cancers that haven’t spread.
Trimodal therapy involves:
- surgery to remove the tumour from the bladder (TURBT)
- radiation therapy combined with chemotherapy (chemoradiation) to destroy remaining cancer cells. People who are not fit enough for chemotherapy will have radiation therapy on its own.
Studies have shown that trimodal therapy has similar outcomes to radical cystectomy for certain small cancers. However, there is a chance the cancer may come back in the bladder and cystectomy may still be required.
Having trimodal therapy – If you have trimodal therapy, chemotherapy or other medicines are given to make the cancer cells more sensitive to radiation. You will usually have radiation therapy as daily treatments, Monday to Friday, over 4–7 weeks as an outpatient.
There are different options for receiving chemotherapy. Some people will have chemotherapy once a week a few hours before or after a radiation therapy session. Other people take a tablet or have an infusion over several days.
During and after chemoradiation, you may have side effects from the chemotherapy and the radiation therapy. The bladder is not removed in trimodal therapy, so you can still urinate in the usual way. You will need to have regular cystoscopies after treatment to check that the cancer has not come back.
Key points about treating muscle-invasive bladder cancer
Surgery
- Surgery is a common treatment for bladder cancer that has invaded the muscle layer.
- A radical cystectomy is the most common surgery for muscle-invasive bladder cancer. It removes the whole bladder and nearby lymph nodes, and often other nearby organs.
Chemotherapy
- Some people will have chemotherapy before or after surgery.
- For systemic chemotherapy, drugs are injected into a vein to treat the cancer; treatment is repeated every few weeks for several months.
Immunotherapy
- This is used before or after surgery. This drug therapy uses the body's own immune system to help fight the cancer.
Radiation therapy
- This uses a controlled dose of radiation to destroy or damage cancer cells.
- It can be given as part of trimodal therapy or on its own for people not fit enough for chemotherapy.
Trimodal therapy
- Trimodal therapy is an alternative to cystectomy. It allows people to keep their bladder.
- It involves a small operation (known as TURBT) to remove the tumour, followed by radiation therapy combined with chemotherapy (chemoradiation).
- After trimodal therapy, people need to have regular check-ups to be sure that the cancer has not come back. This involves having a cystoscopy. If cancer returns, people may need to have a radical cystectomy.
Urinary diversion
If you have surgery to remove the bladder (radical cystectomy), you will need another way to collect and store urine. This is known as a urinary diversion. It is a major change, and your treatment team will offer support to help you adjust.
Your surgeon will talk to you about the best type of urinary diversion for you. They will recommend one of the following options:
- urostomy – creates a new opening to your urinary system
- neobladder – creates a new bladder from your small bowel
- continent urinary diversion – creates a pouch from your small bowel to hold urine until you are ready to drain it.
Urostomy
Also known as an ileal conduit, a urostomy is the most common type of urinary diversion. In a urostomy, urine will drain into a bag attached to the outside of the abdomen. The surgeon will use a piece of your small bowel (ileum) to create a passageway (conduit). This connects the ureters (the tubes that carry urine from your kidneys) to an opening created in the abdomen. The opening is called a stoma.
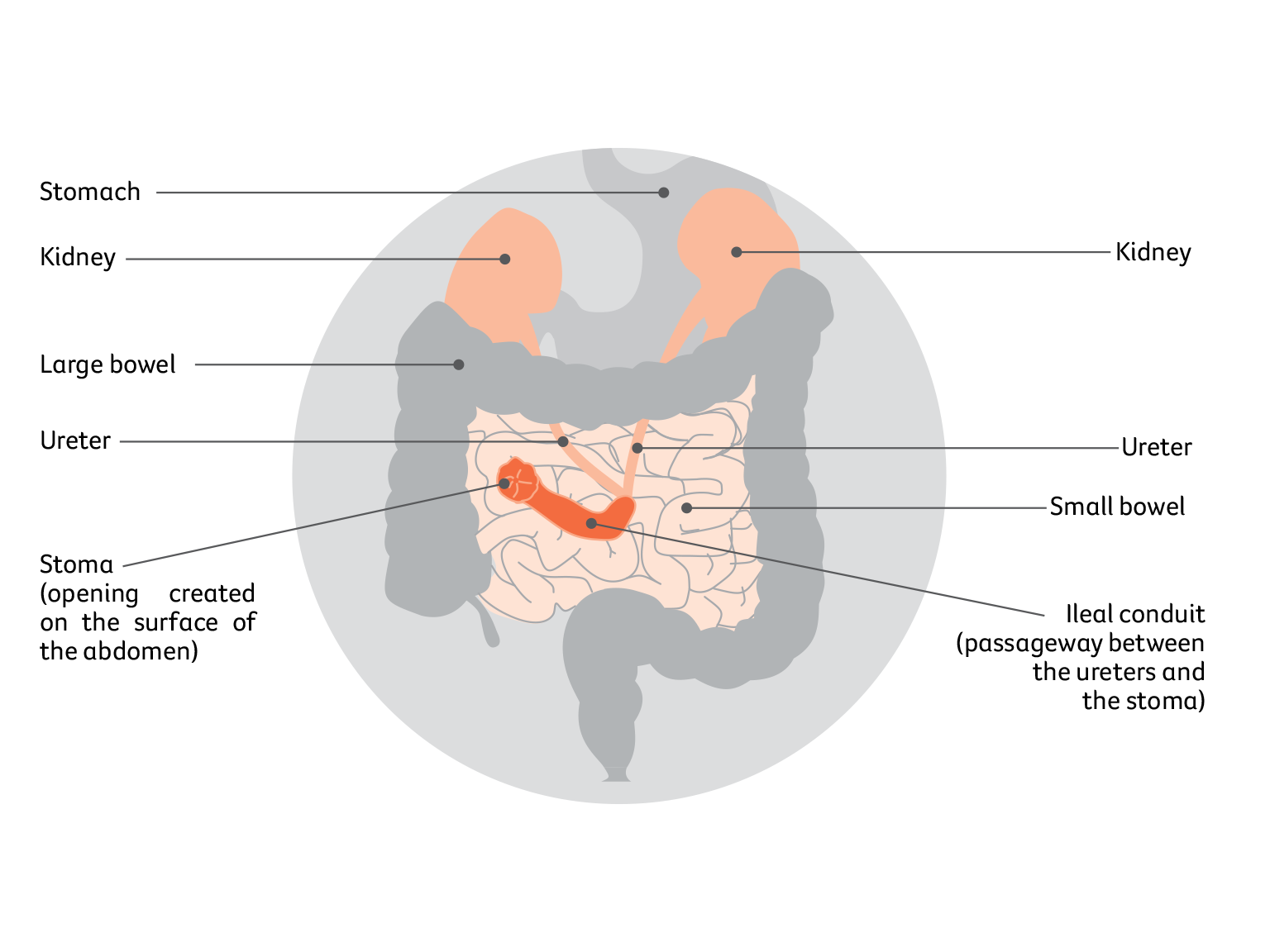
How the stoma works
A watertight, drainable bag is placed over the stoma to collect urine. The bag has an adhesive backing that sticks to your abdomen. This small bag is worn under clothing, fills continuously and needs to be emptied several times a day through a tap or bung on the bag. The small bag will be connected to a larger drainage bag at night if required.
Positioning the stoma
Before the operation, the surgeon and/or a stomal therapy nurse will plan where the stoma will go. They will discuss the position with you and aim to place the stoma so it doesn’t move when you sit, stand or move. Sometimes the position can be tailored for particular needs. For example, golfers may prefer the stoma to be placed so that it doesn’t interfere with their golf swing. The stoma will usually be created on the abdomen, to the right of the belly button.
Having a stoma
For the first few days after the operation, the stomal therapy nurse will look after the stoma and make sure the bag is emptied and changed as often as necessary.
Once you are ready, the stomal therapy nurse will teach you and/or your carer/family member how to care for the stoma. At first, the stoma will be slightly swollen and it may be several weeks before it settles down. The stoma may also produce a thick, white substance (mucus), which might appear as pale threads in the urine. The amount of mucus will lessen over time, but it won’t disappear completely.
Stents (small plastic tubes) will be used to help with the flow of urine while the ureters heal. These stents are placed at the time of surgery and are temporary. They will be removed before you are discharged from hospital, or up to 3 weeks after surgery. Your surgeon will talk to you about when the stents will be removed.
Attaching the bag – There are different types of bags (sometimes called appliances) and the stomal therapy nurse will help you choose one that suits you. The nurse will show you how to clean your stoma and change the bags. This will need to be done regularly, usually every day while in hospital (for teaching purposes) and every 2–3 days after that. It might be helpful to have a close relative or friend join you when the nurse gives the instructions so they can support you at home.
Emptying the bag – How often you need to empty a bag is affected by how much you drink. Staying hydrated is very important with a urostomy. The first few times you empty the bag, allow yourself plenty of time and privacy so that you can work at your own pace without any interruptions.
Living with a stoma
Having a urostomy is a major change and many people feel overwhelmed at first. It’s natural to worry about how the urostomy will affect your appearance, lifestyle and relationships.
Learning to look after the urostomy may take time and patience. It may sometimes affect your travel plans and social life in the early days while you are gaining confidence, but these issues can be managed with planning. After you learn how to take care of the stoma, you will find you can still do your regular activities.
You may worry about how the bag will look under clothing. Although the urostomy may seem obvious to you, most people won’t know you are wearing a bag unless you tell them about it. Modern bags are usually flat and shouldn’t be noticeable under clothing.
After bladder surgery, you may have some physical changes that affect your sex life. You may worry about being rejected or having sex with your partner. If you meet a new partner during or after treatment, it can be difficult to talk about your experiences, particularly if your sex life and body image have been affected.
Sexual intimacy may feel awkward at first, but open communication usually helps. Many people find that once they talk about their fears, their partner is understanding and supportive, and they can work together to make sexual activities more comfortable.
Support for people with a stoma
See a stomal therapy nurse – Stomal therapy nurses are trained in helping people with stomas. They will:
- arrange for you to speak with another person living with a stoma
- answer your questions about the surgery and side effects, including the impact on sexual activities and intimacy
- help you adjust to having a stoma and regain your confidence
- assist you with fitting and using urostomy bags
- give you written instructions on caring for your stoma
- provide ongoing care and support once you are home.
Stomal therapy nurses work in many hospitals. Before you leave hospital, the nurse will make sure that you feel comfortable changing the urostomy bag and that you have a supply of bags.
If your hospital doesn’t have a stomal therapy nurse, your treatment team can help you find one. Or you may be able to find a nurse near you by visiting the Australian Association of Stomal Therapy Nurses (AASTN) at stomaltherapy.au. Your doctor may also be able to arrange for a community nurse to visit you.
Join a stoma association – Your stomal therapy nurse will usually help you join a stoma association. For a small annual fee, you will be able to get support, free bags and related products. Visit the Australian Council of Stoma Associations at australianstoma.com.au.
Register for the Stoma Appliance Scheme – The Australian Government’s Stoma Appliance Scheme (SAS) provides free stoma bags and related products to people who have a stoma. To be eligible, you must have a Medicare card and belong to a stoma association. For details, visit health.gov.au and search for “Stoma Appliance Scheme”.
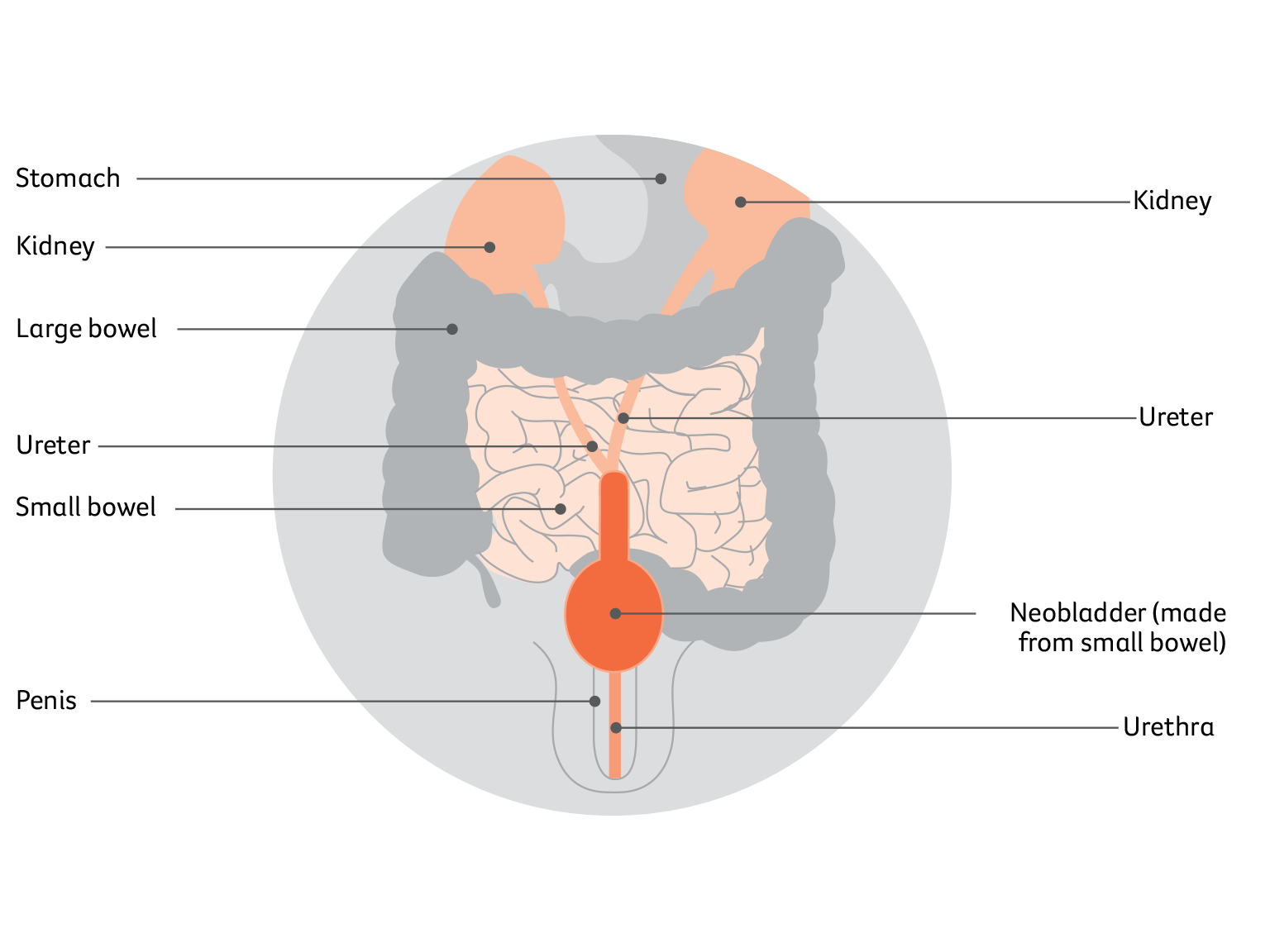
Neobladder
In this method, a pouch is created from a portion of your small bowel and placed in the same area as your original bladder. This pouch is called a neobladder. The procedure for creating a neobladder is more complex and takes longer than creating a urostomy. However, you don’t need to have a stoma with a neobladder.
Once the neobladder is created, the surgeon will stitch it into the ureters to collect and store urine from the kidneys. It will also be stitched into the urethra to drain urine from the body. The neobladder will allow you to urinate through your urethra, but it will feel different from urinating with a normal bladder.
I couldn’t control the number of urinary tract infections after my surgery, but once I started catheterising, it limited the infections.”
Mark
Living with a neobladder
It takes time to get used to a new bladder. The neobladder will not have the nerves that tell you when your bladder is full, and you will have to learn new ways to empty it.
The neobladder may produce a thick white substance (mucus), which might appear as pale threads in the urine. The amount of mucus will lessen over time, but it won’t disappear completely.
Discuss any concerns with your nurse, physiotherapist, GP or urologist, and arrange follow-up visits with them.
See a continence nurse or a pelvic health physiotherapist – They will work with you to develop a toilet schedule to train your new bladder. At first, the new bladder won’t be able to hold much urine and you will probably need to empty your bladder every 2–3 hours. This will gradually increase to 4–6 hours, but it may take several months. During that time, the neobladder may leak when full, and you may have to get up during the night to go to the toilet.
Strengthening the pelvic floor muscles before and after surgery will help you control the neobladder. A continence or pelvic health physiotherapist can teach you exercises.
It can sometimes be difficult to fully empty the neobladder using your pelvic floor muscles. If this is an issue, a continence nurse will also teach you how to drain the bladder with a catheter. This is called intermittent self-catheterisation and it should usually be done twice a day to reduce the risk of urinary tract infections.
Ask about the Continence Aids Payment Scheme (CAPS) – This scheme is operated by Services Australia (Medicare) and provides a payment to eligible people who need a long-term supply of continence aids, including catheters for draining the bladder. You can ask the continence nurse if you’re eligible. Visit servicesaustralia.gov.au to find out more, or call the CAPS team on 1800 239 309.
Contact the National Continence Helpline – Call 1800 33 00 66 to speak to a nurse continence specialist or visit continence.org.au for more information.
Continent urinary diversion
In this procedure, the surgeon uses a piece of the small bowel to create a pouch inside the body. The pouch is designed so that it does not leak urine, but can be drained by inserting a catheter through a stoma. Several times a day you will need to drain the urine by inserting a drainage tube (catheter) through the stoma into the pouch.
This diversion procedure is not commonly used, but may be an option in some circumstances. Your surgeon or nurse will explain the risks and benefits of this procedure, and how to empty urine from the pouch.
Sources and references
Acknowledgments
This edition has been developed by Cancer Council NSW on behalf of all other state and territory Cancer Councils as part of a National Cancer Information Subcommittee initiative. We thank the reviewers of this booklet: Dr Malinda Itchins, Thoracic Medical Oncologist, Royal North Shore Hospital and Chris O’Brien Lifehouse, NSW; Dr Cynleen Kai, Radiation Oncologist, GenesisCare, VIC; Dr Naveed Alam, Thoracic Surgeon, St Vincent’s Hospital, Epworth Richmond, and Monash Medical Centre, VIC; Helen Benny, Consumer; Dr Rachael Dodd, Senior Research Fellow, The Daffodil Centre, NSW; Kim Greco, Specialist bladder Cancer Nurse Consultant, Flinders Medical Centre, SA; Caitriona Nienaber, 13 11 20 Consultant, Cancer Council WA; Marco Salvador, Consumer; Janene Shelton, bladder Foundation Australia – Specialist bladder Cancer Nurse, Darling Downs Health, QLD; Prof Emily Stone, Respiratory Physician, Department of Thoracic Medicine and bladder Transplantation, St Vincent’s Hospital Sydney, NSW; A/Prof Marianne Weber, Stream Lead, bladder Cancer Policy and Evaluation, The Daffodil Centre, NSW. We would also like to thank the health professionals, consumers and editorial teams who have worked on previous editions of this title.

Bladder cancer
Cancer Council 13 11 20
Call us to talk to a specially trained health professional for free and confidential support and information.