
Last updated:
Sources and references 
The type of surgery your doctor suggests will depend on the type and stage of the cancer, where it is in the breast, the size of your breast, and what you prefer. In most cases, you will have one or more lymph nodes removed from the armpit (called axillary surgery).
Some people also choose to have a new breast shape made during the operation, known as breast reconstruction.
The 2 different types of surgery used for breast cancer are:
- breast-conserving surgery – when only part of the breast is removed
- mastectomy – when the whole breast is removed.
Depending on your situation, you may have a choice between the 2 types of surgery. Research has shown that for most early breast cancers, having breast-conserving surgery followed by radiation therapy works just as well as a mastectomy.
The operations have different benefits, risks and side effects.
Talk to your doctor about the best option for you.
Treatment before surgery
While surgery is often the main treatment for both early and locally advanced breast cancer, you may have other treatments before surgery. Called neoadjuvant treatment, it may be discussed at a multidisciplinary team meeting. Chemotherapy is often used before surgery (neoadjuvant chemotherapy or NAC). Or, you may have hormone therapy, targeted therapy or immunotherapy, or a combination of these treatments. Neoadjuvant treatment can help to reduce the size of the cancer before surgery and improve your chance of having a good outcome.
It may also mean you can have less complex surgery. For locally advanced breast cancer, for example, neoadjuvant treatment may mean you can choose to have breast-conserving surgery rather than a mastectomy. In some cases – particularly for people with HER2+ or triple negative cancers – neoadjuvant treatment can kill all cancer cells. Called a complete pathological response, it improves the chance of a good outcome. Ask your doctor if neoadjuvant treatment is an option for you. People with early breast cancer may find the Neoadjuvant Patient Decision Aid helpful. Visit myneoguide.com. After surgery, you may have radiation therapy, chemotherapy, hormone therapy, targeted therapy or immunotherapy. This is called adjuvant treatment. It helps to destroy any cancer cells that remain after surgery.
Breast-conserving surgery
Removing only part of the breast is called breast-conserving surgery. It is also known as a lumpectomy or wide local excision. The surgeon removes the tumour and some of the healthy tissue around it, so that you can keep as much of your breast as possible. The operation will leave a scar, and it may change the size and shape of the breast and the position of the nipple.
Pathology tests on breast tissue
A pathologist looks at the removed tissue under a microscope to check for an area of healthy cells around the cancer (called a clear margin). The pathologist will also give information about:
- the size and grade of the cancer
- whether the cells are hormone receptor positive and/or HER2+ or triple negative
- whether the cancer has spread to any lymph nodes.
If your removed tissue shows multiple cancers, each cancer will be tested separately. The pathology report will help your doctors work out what other treatment may be best for you. If there are cancer cells found close at the edge of the tissue (which is called an involved or positive margin), there is a higher risk of the cancer returning.
You may need to have further surgery to remove more tissue (called a re-excision or wider excision). Your doctor may also suggest that you have a mastectomy.
After having breast-conserving surgery, you will usually then have radiation therapy to destroy any cancer cells that may be left in the breast or armpit.
Mastectomy
Surgery to remove the whole breast is called a mastectomy. One breast may be removed (single or unilateral mastectomy) or both breasts (double or bilateral mastectomy). A mastectomy may be recommended if:
- there is cancer in more than one area of the breast
- the cancer is large compared with the size of the breast
- it is difficult to get a clear margin around the tumour
- you have inflammatory breast cancer
- you have had radiation therapy to the same breast before and so cannot have it again
- the cancer has come back or you have a new cancer in the same breast
- you have the BRCA1 or BRCA2 gene mutation.
You may prefer to have a mastectomy instead of breast-conserving surgery – even if you have a very small cancer. You will not usually have radiation therapy after a mastectomy, although it may be offered in some situations.
The nipple is often removed in a mastectomy. In some cases, however, the surgeon may perform a skin-sparing or nipple-sparing mastectomy. This means that more of the normal skin (with or without the nipple) is kept. If you have decided to have a reconstruction, and can have a skin-sparing or nipple-sparing mastectomy, the reconstruction is sometimes done at the same time.
If you don’t have a reconstruction, you have the option of wearing a soft breast form with a specially designed bra while your surgical wound heals. Breast Cancer Network Australia (BCNA) provides a free bra and temporary soft form. Speak to your breast care nurse for more details. After the wound has healed and the area is comfortable, you have the option to be fitted for a permanent breast prosthesis.
Breast reconstruction
Breast reconstruction is surgery to make a new breast shape (also called a breast mound). There are different ways to construct a breast shape. It can be done using:
- implants
- a flap of your own skin, fat or muscle (an autologous reconstruction)
- a breast implant and your own tissue.
A breast reconstruction can be done at the same time as a mastectomy (immediate reconstruction); or you may prefer to wait for several months or years before having a reconstruction (delayed reconstruction). If you are not having an immediate reconstruction but might consider it in the future, discuss this with your surgeon before surgery. This will help them to plan the mastectomy.
Some people decide not to have a reconstruction and prefer to “go flat”, while others choose to wear a breast prosthesis.
Removing lymph nodes
Cancer cells that spread from the breast usually first spread to the axillary lymph nodes, which are in and around the armpit. Removing some or all of these lymph nodes helps your doctor to check for any cancer spread. The operation to remove lymph nodes is called axillary surgery. It is usually done during breast surgery but may be done in a separate operation. There are 2 main types of axillary surgery.
Sentinel lymph node biopsy (SLNB)
When breast cancer spreads outside the breast, it first goes to a particular lymph node or nodes in the armpit or near the breastbone (sternum). These are called the sentinel nodes. A sentinel node biopsy finds and removes them so they can be tested for cancer cells.
If there are no cancer cells in the sentinel nodes, no more lymph nodes are removed. If there is more than a small amount of disease in the sentinel nodes, you may have axillary lymph node dissection or radiation therapy.
Axillary lymph node dissection (ALND)
If cancer is found in the lymph nodes, then most or all of the axillary lymph nodes (usually 10–25) may be removed to reduce the risk of the cancer coming back (recurrence) in the armpit. The nodes are tested and the results guide what other treatment may be needed. ALND is also called axillary lymph node clearance (AC). Radiation therapy may be used instead of ALND.
Side effects
You may have arm or shoulder stiffness, weakness and pain; numbness in the arm, shoulder, armpit and parts of the chest; fluid collecting near the surgical scar (seroma); lymphoedema; and cording. Side effects are usually worse after ALND than after an SLNB because more lymph nodes are removed in an ALND.
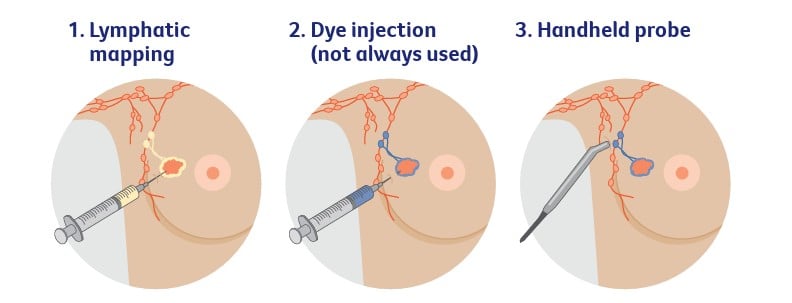
Finding the sentinel nodes
To work out which lymph nodes are sentinel nodes, one or a combination of these procedures is used:
- Lymphatic mapping
A small amount of a harmless radioactive solution is injected into the skin over the breast cancer tumour. A CT scan is then taken to show which lymph nodes the radioactive solution flows to first. These are most likely to be the sentinel nodes. Lymphatic mapping is done either the day before or on the day of the surgery. - Dye injection (not always used)
If dye is being used, it will be injected into the breast. The dye, which may be blue or green, moves into the lymphatic vessels and stains the sentinel nodes first. This is done under general anaesthetic during the surgery.
Because of the dye, you may notice blue-green urine (wee) and bowel movements (poo) when you go to the toilet the next day. You may also have a blue patch on the breast for weeks or longer. Your skin may look a bit grey but will fade once the dye washes out in your urine. - Handheld probe
As well as looking at where the dye travels to first (if used), the surgeon uses a small handheld device called a probe during the surgery to detect the radioactive solution injected during the lymphatic mapping.
This helps to check that the sentinel nodes have been located and the surgeon can then remove them for testing.
What to expect after surgery
If you have any questions about your recovery and how best to look after yourself when you get home, ask the doctors and nurses caring for you. If you are referred to a breast care nurse, they can give you information about what to expect after surgery and provide support.
Your hospital stay will depend on the surgery you have and how well you recover:
- breast-conserving surgery – you usually go home the same day, or may stay overnight
- mastectomy – you usually stay in hospital for 1–2 nights
- reconstruction after mastectomy – you usually stay in hospital for several days.
Managing dressings and tubes
A dressing will cover the wound to keep it clean. This may be changed while you are in hospital but is usually removed after about a week. You may have one or more drainage tubes to drain fluid from the surgical site into a bottle. These can stay in place for up to one week, or occasionally 2 weeks. Nurses will show you how to look after the wound and drainage tubes at home, or a community nurse, GP or your surgeon may help you. If you notice redness or discharge around the surgical area or develop a fever over 38°C, let your treatment team know immediately.
Recovery time
The time it takes to recover from surgery will depend on the type of surgery you have had and your health. You may feel better after a few days, or it may take several weeks or longer if you have had a mastectomy with a reconstruction.
Avoid heavy lifting
Do not do vigorous physical activity or heavy lifting in the initial weeks after surgery. Your treatment team will let you know when you can resume normal activities. You may be given some gentle exercises to reduce the risk of shoulder stiffness.
Shower carefully
Keep the wound clean, and gently pat it dry after showering. Avoid baths.
Manage pain
While in hospital, you will have pain relief through a drip (intravenous or IV), an injection or as tablets. You will also be given pain medicine when you go home. You are likely to need stronger pain relief after an ALND or a mastectomy than after breast-conserving surgery.
Apply moisturiser
Gently massage the area with moisturiser once any stitches or adhesive strips are removed and the wound has completely healed. About 6 weeks after surgery, your surgeon may suggest that you use silicone gels and sheets to reduce scarring.
Avoid cuts
Your treatment team may advise you to wait until the wound has completely healed if you want to shave or wax your armpits.
Prevent blood clots
While in bed, you should try to do some deep breathing exercises, and move your legs around to help prevent blood clots in the deep veins of your legs (deep vein thrombosis or DVT). As soon as you are able, you will be asked to get up and walk around. You may wear elastic (compression) stockings or use other devices to help prevent clots. Your doctor might prescribe medicine that reduces the risk of blood clots forming.
What your breast looks like after surgery
How your breast will look after surgery depends on the type of surgery that you have, as well as the size of your breast and your body shape. It can take up to a few weeks for any bruising and swelling of the surgery area to go away.
After breast-conserving surgery
The size and position of the scar will depend on how much tissue was removed. The scar will usually be less than 10 cm and near where the cancer was or around the areola or near the breast fold. But this can vary depending on your breast size and how much breast tissue needs to be removed. It can also change if you need to have further surgery to remove more tissue. If a larger area needs to be removed, surgical techniques known as oncoplastic surgery can reshape the breast after breast-conserving surgery.
After a mastectomy
The scar will be across the skin of the chest. If you have surgery to remove the lymph nodes, the scar will also be in the armpit. At first the scar will be firm, slightly raised and red. Over the next few months, it will flatten and fade.
Impact on self-esteem
Scars or changes to how your breast looks can affect how you feel about yourself (self-image and self-esteem). If you have had a mastectomy (or part of your breast removed), it’s common to feel a sense of loss. It may also affect your sense of identity.
Seeking support
Talking to someone who has had breast cancer surgery can be helpful. Cancer Council’s Cancer Connect program may be able to link you to others who have had a similar experience. Speaking with a counsellor or psychologist for emotional support and coping strategies can also help. Call Cancer Council 13 11 20 for details.
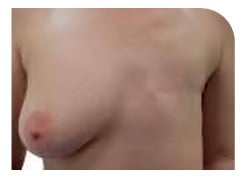
Breast appearance after surgery
What your breast will look like after surgery varies from person to person. It will depend on the type of surgery you have and how much tissue is removed. The pictures below give some examples of how your breast might look but ask your surgeon for more photographs to help you choose the best approach for you.

Breast-conserving surgery
Two years after surgery to left breast. The scar can still be seen but has healed and faded a little. The size of the scar varies but can be around 10 cm. The surgery was followed by radiation therapy.
Mastectomy
Left breast removed, with no reconstruction. All possible breast tissue has been removed and the scar runs horizontally across the chest wall. This photo is some time after surgery and shows results once the scar has healed.

Nipple-sparing mastectomy with an implant reconstruction
Left breast removed with a nipple-sparing mastectomy, followed by a breast reconstruction using an implant. If it is not possible to keep the nipple, there is the option of having a nipple reconstruction later.

Mastectomy with a flap reconstruction
Right breast removed, followed by a breast reconstruction using tissue from the back. Tissue from the abdomen, buttock or thigh can also be used for a reconstruction. You can choose to have a nipple reconstruction later.
Side effects of surgery
Some common side effects are discussed below. Talk to your treatment team about the best ways to deal with them. For more information, visit Managing side effects.
Fatigue
Cancer treatment and the emotional impact of the diagnosis can be tiring. Fatigue is common and may continue for weeks or months. Research shows that exercise during and after cancer treatment is safe and can help improve fatigue. Cancer Council may run an exercise program near you – call 13 11 20. You can also ask your GP if you are eligible for some Medicare-funded sessions with an exercise physiologist or a physiotherapist.
Shoulder stiffness
Arm and shoulder pain, weakness, stiffness and reduced movement are common after surgery and after radiation therapy. Ask your treatment team when you can start exercising your arm. A physiotherapist or exercise physiologist can show you exercises to reduce shoulder stiffness or pain. This may help prevent lymphoedema.
Numbness and tingling
Surgery can bruise or injure nerves. You may feel numbness and tingling in the armpit, upper arm or chest area. You may also notice a loss of feeling in your breast or nipple. These changes often improve within a few weeks but may take longer. Sometimes the numbness or tingling may not go away completely. A physiotherapist or occupational therapist can give you exercises that may help.
Seroma
Fluid may collect in or around the surgical scar and cause a balloon-like swelling. This is most common after a mastectomy. A seroma can also develop in the armpit after an ALND. The build-up of fluid can be uncomfortable but is not harmful. Some breast care nurses, your specialist or GP, or a radiologist can drain the fluid using a fine needle and a syringe. This procedure is not painful, but it may need to be repeated over a few appointments.
Lymphoedema
Fluid building up in the tissue of the arm or breast may cause swelling after any lymph node surgery. It is common to have some swelling of your arm or breast after surgery, but this usually settles in the weeks afterwards. If this swelling builds up over weeks or months, this usually means you have lymphoedema. It can happen any time, even years after surgery (or radiation therapy) to the lymph nodes.
Post-mastectomy pain
It is rare to have prolonged pain after a mastectomy but you may find the scar uncomfortable for some time. If pain or discomfort is ongoing, let your treatment team know.
Cording
Also known as axillary web syndrome, cording is caused by hardened lymph vessels. It feels like a tight cord running from your armpit down the inner arm, sometimes to the palm of your hand. Find out how to manage cording.
Find out more about the types of treatments:
Sources and references
This information has been developed by Cancer Council NSW on behalf of all other state and territory Cancer Councils and Cancer Council Australia as part of a National Cancer Information Subcommittee initiative. We thank the reviewers of this content: Dr Diana Adams, Medical Oncologist, Macarthur Cancer Therapy Centre, NSW; Prof Bruce Mann, Specialist Breast Surgeon and Director, Breast Cancer Services, The Royal Melbourne and The Royal Women’s Hospitals, VIC; Dr Shagun Aggarwal, Specialist Plastic and Reconstructive Surgeon, Prince of Wales, Sydney Children’s and Royal Hospital for Women, NSW; Andrea Concannon, consumer; Jenny Gilchrist, Nurse Practitioner Breast Oncology, Macquarie University Hospital, NSW; Monica Graham, 13 11 20 Consultant, Cancer Council WA; Natasha Keir, Nurse Practitioner Breast Oncology, GenesisCare, QLD; Dr Bronwyn Kennedy, Breast Physician, Chris O’Brien Lifehouse and Westmead Breast Cancer Institute, NSW; Lisa Montgomery, consumer; A/Prof Sanjay Warrier, Specialist Breast Surgeon, Chris O’Brien Lifehouse, NSW; Dr Janice Yeh, Radiation Oncologist, Peter MacCallum Cancer Centre, VIC. We also thank the health professionals, consumers and editorial teams who have worked on previous editions of this title.
Photographs have been reproduced with permission from A/Prof James French, Westmead Breast Cancer Institute, NSW; Prof Elisabeth Elder, Westmead Breast Cancer Institute and The University of Sydney, NSW; and Breast Cancer: Taking Control, breastcancertakingcontrol.com © Boycare Publishing, 2010.

Breast Cancer
Cancer Council 13 11 20
Call us to talk to a specially trained health professional for free and confidential support and information.
Guide to best cancer care
This breast cancer guide explains the standard of high-quality cancer care that all Australians can expect, from diagnosis, to treatment, recovery, and living with cancer.