
Head and neck cancers
Managing side effects of head and neck cancers
Head and neck cancer treatments can cause side effects. Many side effects can be managed with medical treatments, lifestyle changes, exercise, and support from healthcare professionals.


Last updated:
Sources and references 
Treatment for head and neck cancer is often difficult both physically and emotionally, and it will take some time to recover. Side effects may be temporary, long-lasting or permanent, and some will need ongoing management and treatment. This chapter has information and tips to help you manage any side effects you may have, including:
- fatigue
- mouth sores, ulcers and dry mouth
- changes to taste, smell and appetite
- swallowing problems, including using a feeding tube
- not getting enough fluids
- malnutrition and weight loss
- changes to how you talk
- breathing changes, including having a breathing tube (tracheostomy) or hole (stoma), and restoring speech
- ongoing pain, numbness and stiffness
- changes to how you look
- impact on your sex life and intimacy
- changes to vision or hearing
- ongoing swelling, known as lymphoedema.
Your treatment team will explain what to expect and side effects to watch for. Tell them about any side effects you have and ask which health professionals may be able to help you to cope.
Fatigue
It is common to feel very tired during or after treatment, and you may lack the energy to carry out day-to-day activities. Fatigue for people with cancer is different from tiredness, as it may not go away with rest or sleep. You may lose interest in things that you usually enjoy doing or feel unable to concentrate on one thing for very long. For some people, fatigue continues for months or years after treatment ends.
Let your treatment team know if you are struggling with fatigue. Sometimes fatigue can be caused by a low red blood cell count or be a side effect of drugs or a sign of depression, which can all be treated. There are often programs available through hospitals and treatment centres to help you manage fatigue. A referral to an occupational therapist can also assist with managing fatigue.
Tips for managing fatigue
- Plan your day. Set small manageable goals and rest before you get too tired.
- Keep to a regular schedule if possible. Avoid sleeping in, go to bed at your usual time, and take a short nap if you get tired during the day.
- Don’t expect to be able to do everything you used to be able to right away. Gradually increase the activity you do each day.
- Eat a healthy, well-balanced diet to keep energy levels up.
- Regular light-to-moderate exercise has been shown to reduce fatigue. Even a walk around the block can help. A physiotherapist or exercise physiologist can make an exercise program for you.
- Ask for and accept help with shopping or childcare. Try apps like Gather My Crew.
Mouth problems
Some cancer treatments cause mouth sores, ulcers and saliva changes, which make eating difficult. But there are ways to manage this.
Mouth sores and ulcers – Also called oral mucositis, sores and ulcers are a common side effect of chemotherapy and radiation therapy. They form on soft tissue in your mouth and make eating, swallowing and talking painful. They usually go away as you recover from treatment.
Your doctor can give you medicines to reduce the pain when you eat, drink or speak. Some pain medicines can be applied directly to the mouth sores to numb them. You may use more than one type of medicine to control the pain. Keep your mouth clean during treatment to lessen the risk of infection. Alcohol-free mouthwashes help keep your mouth as clean as possible.
Ask your speech pathologist and dietitian what to eat. Try soft, smooth and cooler foods or nourishing fluids, and avoid acidic or spicy foods. If you can’t eat and drink enough, you may need a temporary feeding tube to support you during treatment and recovery.
Dry mouth and saliva changes – Radiation therapy to the head or neck area and surgery that affects the salivary glands can reduce the amount of saliva in your mouth, make your mouth dry or make your saliva thick and sticky. Known as xerostomia, this is often long-lasting.
Xerostomia can make chewing, swallowing and talking difficult. A dry mouth can also make it harder to keep your teeth and mouth clean, and can increase the risk of tooth decay. Be careful to keep your mouth and teeth clean and have regular dental checks.
How to relieve mouth problems
Mouth sores and ulcers
- Rinse your mouth often – when you wake up, after you eat, and at bedtime. Ask your doctor or nurse what alcohol-free mouthwash to use. They may suggest a homemade mouthwash or a specific mouthwash to help with mouth ulcers.
- Talk to your doctor and nurse about medicines to relieve pain and help with healing.
- Use a soft toothbrush and replace it often to reduce the risk of infections. Brush gently after meals and before bed. If brushing is too painful, try using a water flosser on a low setting.
- Suck on ice cubes.
- Avoid rough, crunchy or dry foods (e.g. chips, toast), vinegar, spices, salty foods, alcohol, very hot or cold things, and citrus, tangy or tomato-based food or juice.
- Use a lip balm for moist lips.
- Tell your doctor, dietitian or speech pathologist if it is hard for you to swallow.
Dry mouth
- Ask your dentist about an oral care plan and have regular check-ups.
- Carry a water bottle and have regular sips throughout the day.
- Limit alcohol and caffeine (these can be dehydrating) and avoid smoking.
- Chew sugar-free gum to help the flow of saliva.
- Put lanolin on your lips (but avoid products containing petroleum).
- Soften food by dipping it into milk or soup, or moisten it with gravy, sauce, cream or custard.
- Drink fluids with meals to help soften the food and make it easier to swallow.
- Acupuncture may help to improve dry mouth. Talk to your doctor before trying it.
- Use artificial saliva, dry mouth gels or lubricating agents from the chemist. Swirl grapeseed oil in your mouth and then spit it out.
Taste, smell and appetite changes
Having treatments to the head, neck andmouth area may affect your sense of taste and smell.
After some surgeries to the nasal cavity, you may lose your sense of smell, and your sense of taste may also be affected. If you have a laryngectomy, air will no longer pass through your nose, which can affect your sense of smell. Surgery to the mouth may also change how food tastes.
Some treatments, especially radiation therapy, can change the way the salivary glands work and affect the flavour of food. Food may taste bitter or metallic, or may not have as much flavour as before.
It is important to try to keep eating well so your body gets enough nourishment to maintain your weight. If you lose most or all of your sense of taste, experiment with different textures and temperatures to make food more enjoyable. You could also focus on other appealing aspects of food, such as the colours and presentation of the meal. Another option is to do something else while eating, such as watching TV or reading a book – this might distract you from the food not tasting like it did before.
It can take several months for your sense of taste and smell to return to normal, and this may affect your appetite. If your sense of smell continues to be affected, a speech pathologist may be able to teach you a technique to help you regain your ability to smell. In some cases, taste changes may be permanent.
How to manage taste and smell changes
Taste
- Add extra flavour with herbs if food tastes bland.
- Rinse your mouth before eating to clean any coating from your tongue and help improve taste.
- After each meal, brush your teeth and rinse with the mouthwash recommended by your treatment team.
- If you smoke, try to quit. Smoking reduces appetite and changes the taste of food. Call the Quitline on 13 7848 for support.
- Use a paper or silicone straw so the taste of drinks isn’t as strong. (Metal straws may add a metallic taste.)
- Add more nutrition and energy to your food by using butter or milk.
- Encourage your appetite with aromatic foods.
- If food tastes “off”, freshen your mouth by drinking a fruit or herbal tea, or eating sorbet or soft fruits such as watermelon.
- Ask to see a dietitian for more suggestions.
Smell
- If you lose your sense of smell, take extra care with safety issues. Check the use-by dates of foods, turn off gas appliances properly, and make sure that the smoke detectors in your
home are working. - If food smells bother you, ask your family and friends to cook for you, or try cold meats and salads, and cold desserts and fruit.
- Choose foods that are fresh and full-flavoured.
- If taste and smell changes stop you eating enough, you may lose weight. Use nutritional supplement drinks (e.g. Sustagen, Ensure, Resource) to help maintain your strength and energy. You can find them in many pharmacies and supermarkets.
- You may also want to see a dietitian for help. Some nutritional supplements, such as Resource 2.0, are only available with a dietitian prescription.
Swallowing difficulties
Your lips, teeth, tongue and the muscles in yourmouth, jaw and throat all work together to help you chew and swallow. Difficulty swallowing (dysphagia) before, during or after treatment is common. This may be because of the cancer or the treatments, and may be shortor long term. Swallowing is important to make sure you eat and drink enough. Signs of swallowing difficulties include: taking longer to chew and swallow; taking longer to eat a meal than your family and friends; coughing or choking while eating or drinking; food sticking in your mouth or throat; or pain when swallowing.
Surgery to the jaw, mouth or throat areas – This may make chewing and swallowing difficult because tissue has been removed or reconstructed, or because the surgery has caused dry mouth.
Surgery to the larynx or pharynx – This may make swallowing difficult and cause food to go down the wrong way and into the lungs (aspiration). (This is unlikely after a laryngectomy.) Signs of aspiration include: coughing during or after swallowing; increased shortness of breath during or after a meal; and recurrent chest infections. A speech pathologist can check how your swallowing is working (see Swallowing test, below) and give you strategies to help you eat and drink safely.
Radiation therapy – This can cause dry mouth, pain, and weaken the muscles and nerves used to swallow. It may be worse if you have chemoradiation (chemotherapy and radiation therapy at the same time).
Swallowing test
You may have a test before and after treatment to look at what happens when you swallow. A speech pathologist uses a movie-type x-ray known as a videofluoroscopic swallow study or modified barium swallow study to check that foods and liquids are going down the correct way. You may also have a test called a fibre-optic endoscopic evaluation of swallowing during a nasendoscopy to see how well you can swallow. The test results will help the treatment team plan how any swallowing issues are treated.
How to eat when swallowing is difficult
- A speech pathologist can help with ways to chew and swallow food. They may suggest changing the consistency of what you eat to ease any pain, to make it easier to swallow or to avoid food going down the wrong way (aspiration). They can show you swallowing and vocal exercises and ways to change your posture that may also be helpful. To find a speech pathologist, ask the team at your treatment centre or visit speechpathologyaustralia.org.au.
- If it’s hard to swallow fluids without choking, a speech pathologist can suggest ways to thicken your supplement drinks. Thicker fluids are easier to control in your mouth, so there is less chance of them going down the wrong way.
- Continue to eat and drink when possible throughout treatment. This will keep your swallowing muscles working and reduce the risk of long-term problems. Even with a feeding tube, eating and drinking small amounts can help with swallow recovery, as long as there is no risk of aspiration.
- Try the recipes in the free online books from Griffith University – From Treatment to Table and Beyond the Blender: Dysphagia Made Easy. You can find them by putting the titles into your web search engine.
- A dietitian can make sure that you are getting enough nutrition and hydration.
- Ask your doctor about medicines, including mouth rinses, that can relieve pain or discomfort.
Using a feeding tube
As a result of surgery or radiation therapy, you may find eating and swallowing uncomfortable or difficult. A feeding tube may be inserted either before, during, or after your surgery or radiation therapy to help you get the nutrition you need. This tube is usually temporary, but sometimes it is permanent.
A feeding tube can help ensure you maintain your weight and energy. It is important to avoid losing a lot of weight during treatment and to have enough kilojoules and fluids. If you can’t swallow medicines, check with your doctor, nurse or pharmacist whether these can also be given through the feeding tube.
Your health care team will explain how to:
- care for the tube to prevent it leaking or becoming blocked
- avoid infections – this may include washing your hands before using the tube, and keeping the tube and your skin dry
- monitor for signs that the tube needs to be replaced
- handle issues such as what to do if the tube falls out – while this is very rare it is important to let your treatment team know immediately
if this happens - ensure the tape is secure, especially after a shower – if it’s not secure, the tube can be accidentally bumped out of place.
If you have a feeding tube, it is still important to brush your teeth and keep your mouth clean even though you are not eating or drinking.
The thought of having a feeding tube can be frightening, and it is common to have a lot of questions. Getting used to a feeding tube takes time. Talking to a dietitian or nurse can help, and a psychologist or counsellor can provide emotional support and suggest ways to cope.
Types of feeding tubes
Temporary feeding tube
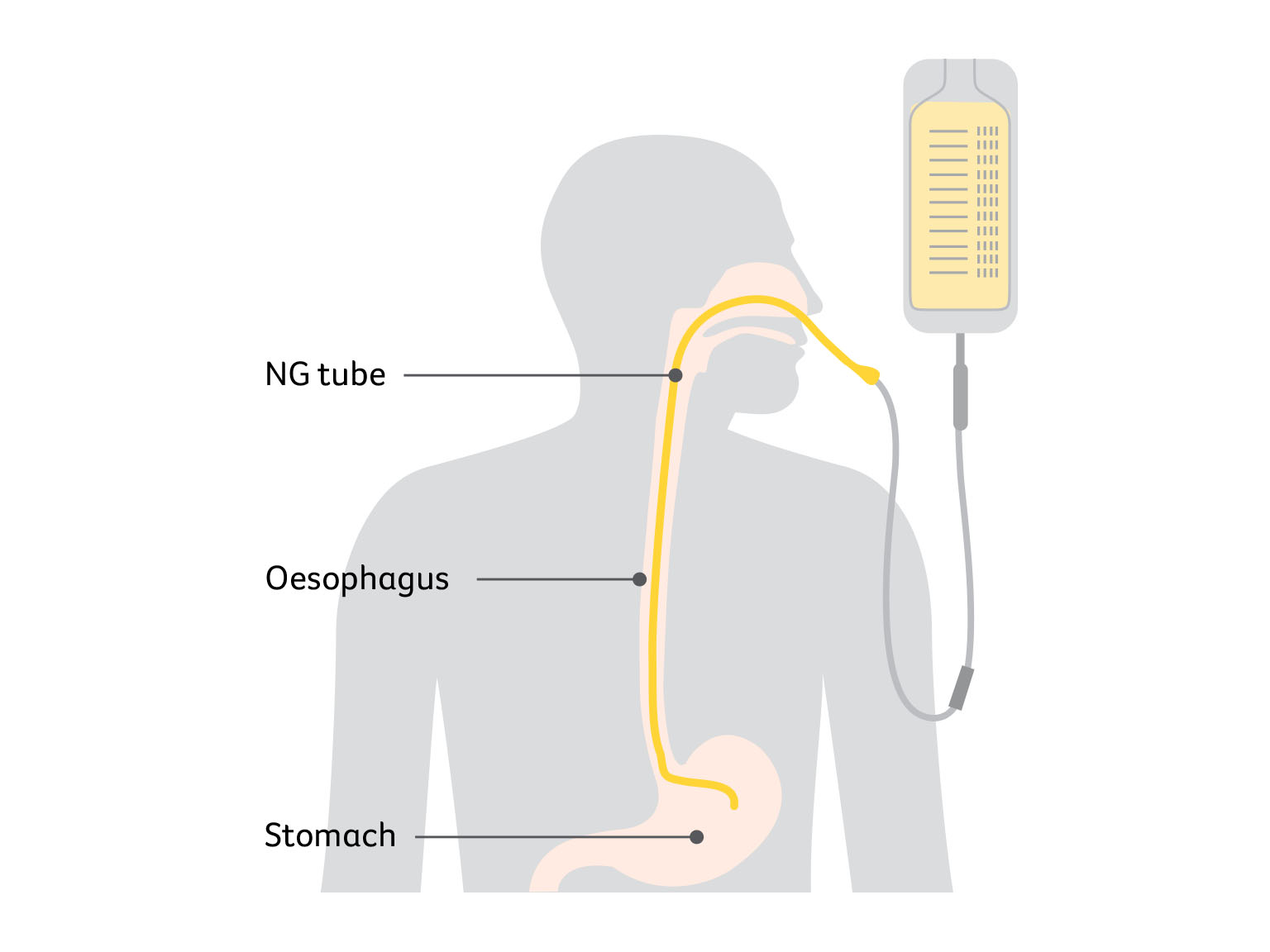
A thin tube is put into a nostril, then down the throat and oesophagus into the stomach. This is called a nasogastric or NG tube. It is mostly used if you need a feeding tube for a short time (e.g. the days or weeks after surgery when you can’t eat).
A doctor may put in an NG tube during an operation when you are asleep. Or a nurse or doctor may put in or remove the NG tube while you’re awake. A spray is usually used to numb the area to make it less uncomfortable to insert the tube. You will be given specially prepared liquid nutrition through this tube.
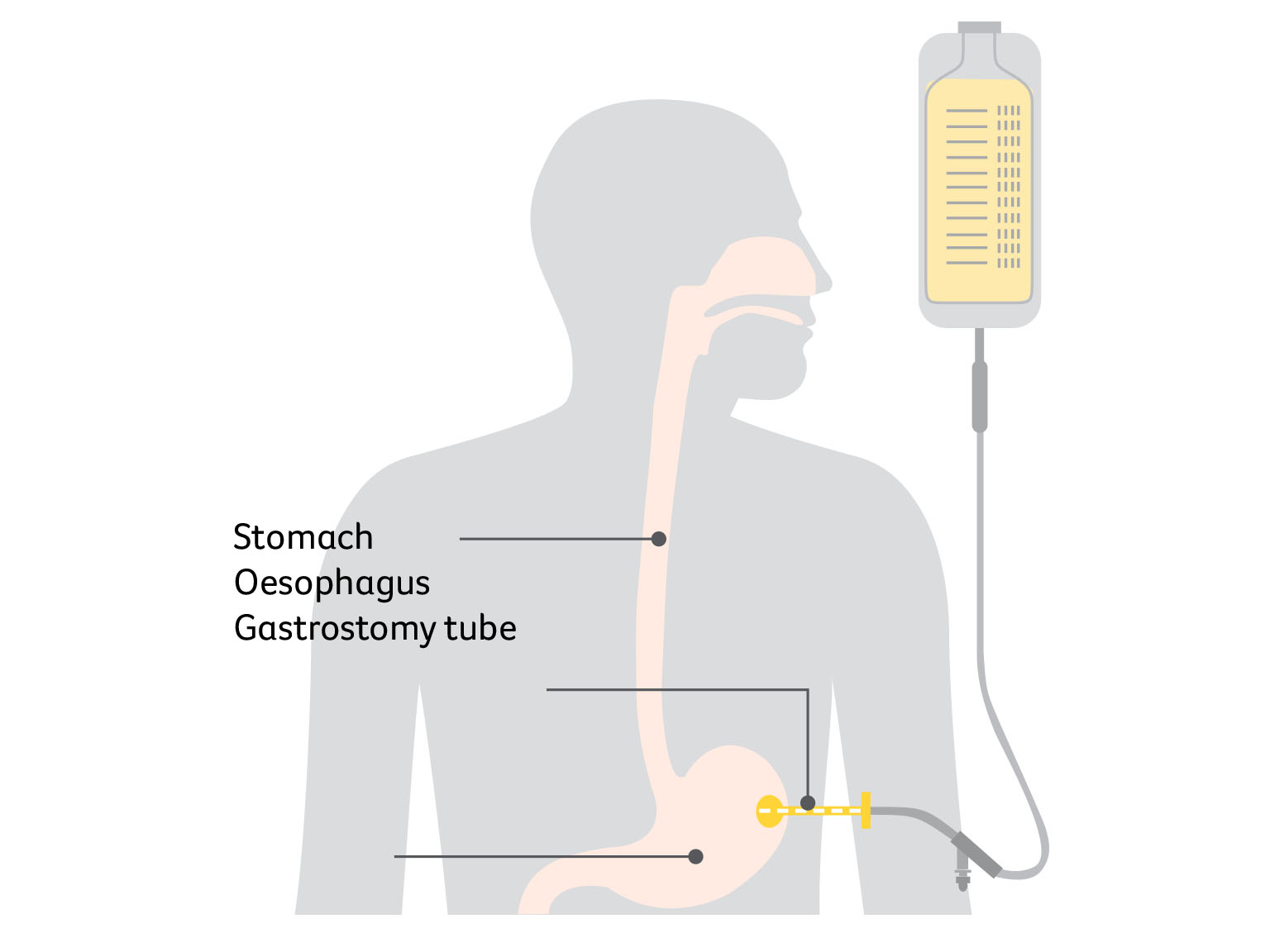
Long-term or permanent feeding tube
A tube is inserted through a hole in your belly into the stomach. This is called a gastrostomy tube. It may be used if you need a feeding tube for a longer time, such as during a recovery period from radiation therapy or after a very big operation.
Depending on the way the tube is inserted, it may be done while you’re awake or under anaesthetic. The tube may be inserted by endoscope (percutaneous endoscopic gastrostomy or PEG tube), using an x-ray (radiologically inserted gastrostomy or RIG tube), or surgically (surgical gastrostomy).
Malnutrition and weight loss
Various side effects may make eating difficult, which can cause you to lose weight. Even a small drop in your weight (e.g. 3–4 kg), especially over a short period of time, may put you at risk of malnutrition. You can be malnourished even if you are overweight.
Unplanned weight loss and malnutrition can reduce your strength, energy and quality of life. This can affect how you respond to treatment, and side effects may be more severe and your recovery slower. During treatment and recovery, a dietitian can assess whether a feeding tube will help you maintain or gain weight.
How to prevent unplanned weight loss
- Treat eating and drinking like medicine: something that you have to do to feel better.
- Eat 5–6 small meals a day rather than 3 large ones.
- Keep a selection of snacks and drinks handy for when you feel up to having them. Keep something in your bag, at work or in the car.
- Try ready-to-use nutritional supplement drinks available from supermarkets and pharmacies (e.g. Sustagen, Ensure, Resource).
- Include high-energy and high-protein foods at every meal or snack. For example, try having milk-based drinks rather than water and choose cheese and biscuits instead of eating lollies.
- Talk to your doctor, nurse or dietitian if you are losing weight, or if you have discomfort or pain when you are swallowing.
Changes to speech
How you talk can be affected by surgery and radiation therapy. This may be because of side effects such as swelling and irritation, because of a tracheostomy or laryngectomy, or because other structures have been removed. You may find it hard to speak clearly or notice your speech is slurred, or your voice may change. The extent of any changes will vary depending on the location of the cancer, how advanced it was, and the treatment you had.
Talking will take time and practice – it’s natural to feel distressed, frustrated and angry at times. You will need to get used to the way your new voice sounds. The National Relay Service can help you make phone calls (visit Access Hub).
How to manage speech changes
- Try non-verbal ways to communicate – gesture, point, nod, smile, mouth words, write things down or ring a bell to call people.
- Use a computer, tablet, phone, text-to-speech apps or notebook to write notes.
- A speech pathologist can improve your speech and offer ways to communicate with family and friends. They may give you some exercises to improve the strength and range of motion of your lips, tongue, jaw and larynx.
- Encourage family and friends to be honest if they don’t understand you and to learn new ways to communicate. Ask them not to avoid conversation even if it is difficult. They need to give you time to respond.
- It can be frustrating and difficult when you can’t communicate. It may help to have someone you trust to advocate for you or explain what you’re trying to say.
- See a counsellor or psychologist if you are finding it difficult to cope.
Breathing changes
Some people treated for head and neck cancer need a tracheostomy. This is an alternative airway created in the front of the neck so they can keep breathing freely.
Having a tracheostomy – If you have a tracheostomy, a small cut in the lower neck allows a tube to be inserted into the windpipe. This can be used for breathing during and after surgery when the mouth or throat becomes swollen. It will also make it easier for you to cough up mucus after a long operation. The tube is usually removed within one week of surgery once the swelling has gone down. In some cases, a tracheostomy is needed for longer than this. It is sometimes needed during radiation therapy, though this is uncommon.
The thought of a tracheostomy may be confronting and scary – talk to your treatment team about how you are feeling and ask them to explain why the tracheostomy is needed. Initially you may not be able to speak, but you will be supported by your treatment team while you have a tracheostomy in place. The speech pathologist and physiotherapist will play an important role in your care.
Once the tracheostomy tube is removed, the hole in your neck normally closes within days. During this time, your voice may be weak and breathy, returning to normal when the hole closes.
Having a laryngectomy – If you have a total laryngectomy, a permanent stoma or breathing hole will be created in your lower neck at the time of the surgery. This will be discussed with you before surgery so you know exactly what to expect, including how you will speak again. If you need a permanent stoma, the speech pathologist and nurses will teach you how to look after it.
Types of alternative airways for breathing
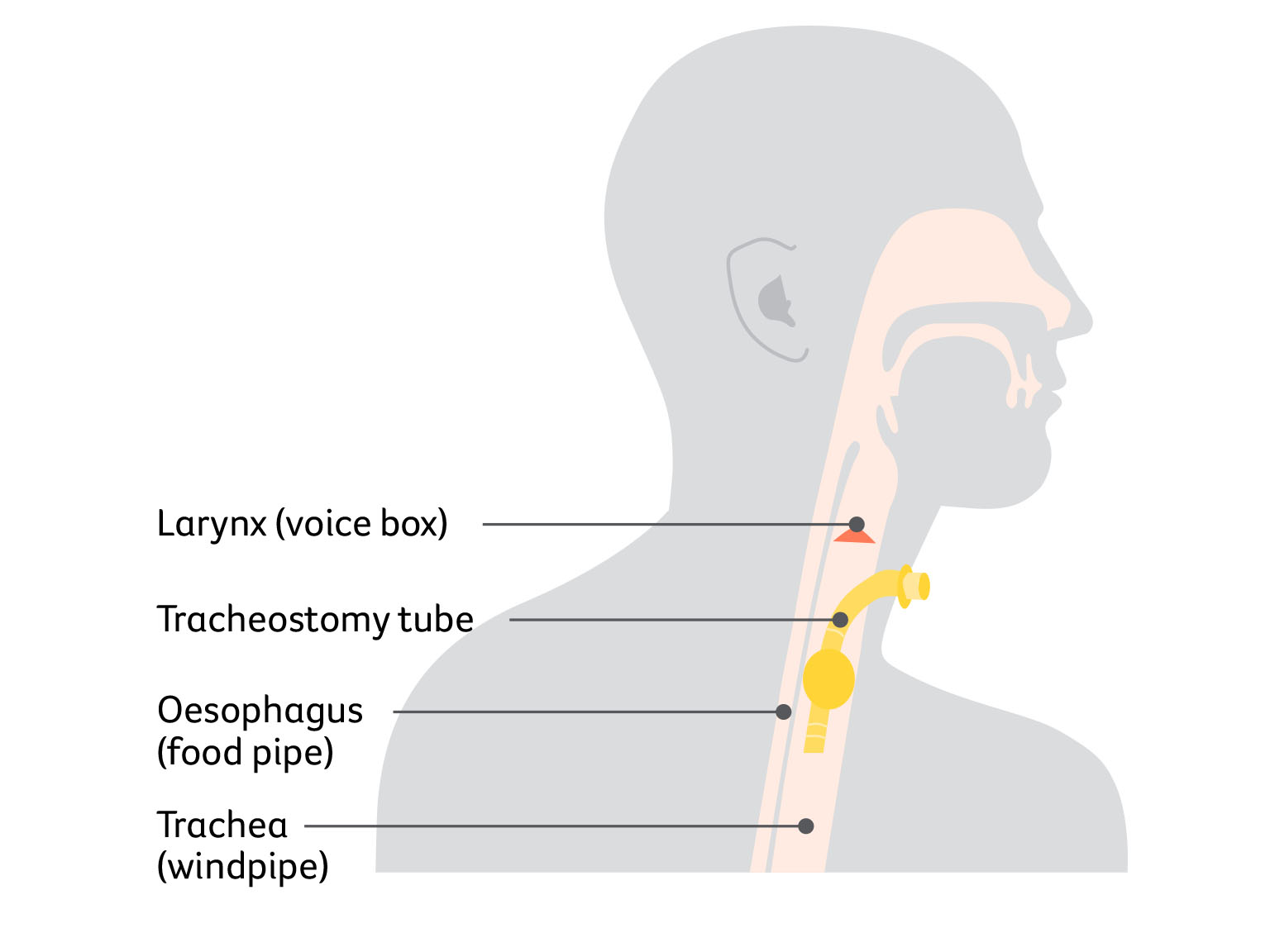
A tracheostomy is a surgically created hole (stoma) in your windpipe (trachea) that provides another airway for breathing. A tracheostomy tube is inserted through the hole, and it may be temporary or permanent.
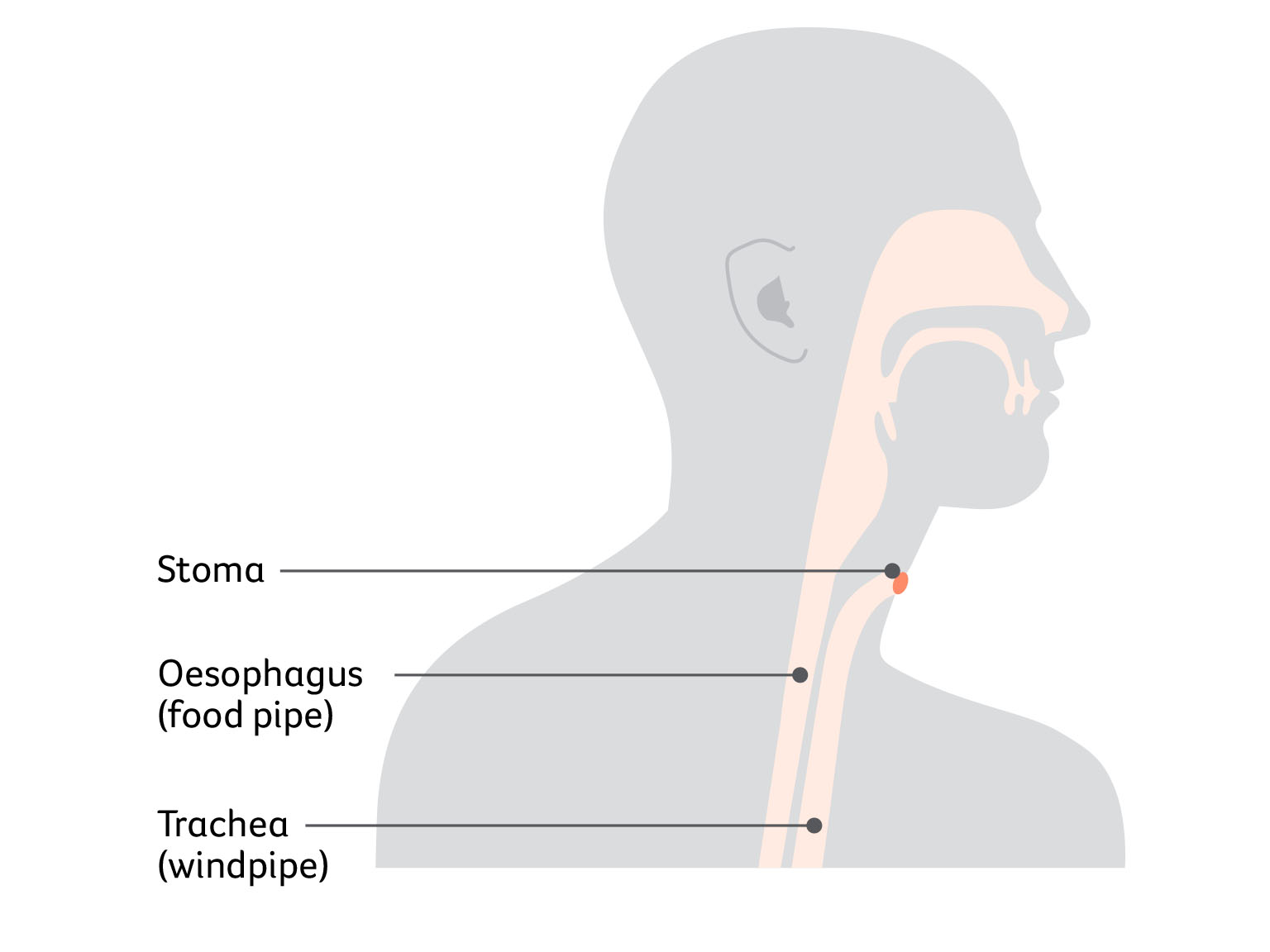
Laryngectomy stoma
A laryngectomy stoma is a permanent opening in your neck that allows you to breathe. It does not require a tube to keep it open, but some people have a laryngectomy tube to stop the hole getting smaller.
Living with a tracheostomy or stoma
Having a tracheostomy or stoma is a big change and takes some getting used to. Your specialist, nurse, physiotherapist or speech pathologist can explain ways to manage the following concerns:
- caring for the tube or stoma – you will be shown how to clean and care for the tracheostomy tube or stoma
- coping with dry air – the air you breathe will be much drier since it no longer passes through your nose and mouth, which normally moistens and warms the air. This can cause irritation, coughing and extra mucus coming out of the tracheostomy tube or stoma. There are products available that cover the stoma or attach to the tracheostomy tube to provide heat and moisture for the windpipe. Your treating team will recommend which option is best for you
- swimming and bathing – you will need to use a special stoma cover to avoid water getting into the windpipe, even in the shower. If you have a laryngectomy stoma, you may not be able to go swimming.
Speaking after a laryngectomy
If the larynx (voice box) is removed, there are various ways to speak.
Voice prosthesis speech – The surgeon makes an opening between your trachea and oesophagus. This is called a tracheoesophageal fistula or puncture. A small voice prosthesis (or valve) is inserted to direct air from your trachea to the oesophagus. This will allow you to speak clearly in a low-pitched, throaty voice.
Mechanical speech – A battery- powered device (electrolarynx) is used to create a mechanical voice. The device is held against the neck or cheek or placed inside the mouth. You press a button on the device to make a vibrating sound.
Oesophageal speech – You swallow air and force it up through your oesophagus to produce a lowpitched sound. This method can be difficult, and you will need training.
Pain, numbness and stiffness
Ongoing pain, numbness and restricted movement in the head and neck area can be upsetting and cause low mood, fatigue or reduced appetite. These can all affect your quality of life. Speak to your treatment team about ways to manage pain and regain movement, which may include medicines, positioning for comfort, exercises and other methods.
Your specialist, cancer care coordinator or GP can suggest other health professionals to see, such as a physiotherapist, occupational therapist, speech pathologist, massage therapist, psychologist or pain specialist.
Nerve damage – If you have lymph nodes removed from your neck, you may have pain and stiffness in your shoulder, or nerve damage that makes your neck feel tight and numb. This may affect how you are able to move your neck or it may make it hard to lift your arm. Partial nerve damage usually heals within 12 months, and feeling should return for many people. In some cases, issues to do with nerve damage are permanent.
Swelling and pain – Some swelling, pain and stiffness in the head and neck area is common after surgery or if you have radiation therapy as your main treatment. This gradually improves with time. Sometimes swelling called lymphoedema can last longer.
Reduced mouth opening – Not being able to fully open the mouth or jaw is called trismus. It can happen after radiation therapy or surgery, and can affect eating, speech and oral hygiene. It may be temporary or permanent. A speech pathologist or physiotherapist can help improve motion, and you can have medicines to reduce pain.
Pins and needles or numbness – Some chemotherapy drugs can cause nerve damage that leads to tingling, pain or numbness in the hands and feet. This is known as peripheral neuropathy and may affect walking or balance. It is often temporary but can be permanent. You may have difficulty feeling things in your hands and feet, or persistent feelings of having cold feet. Let your treatment team know about any tingling, pain or numbness, as there are ways to manage these symptoms.
Changes to appearance
Many types of surgery for head and neck cancer will cause temporary or permanent changes to the way you look.
Weight loss – It is common to lose weight during treatment and many people find it hard to put the weight back on.
Feeding tubes and stomas – People who need a feeding tube or tracheostomy tube or who have a stoma following a laryngectomy may feel self-conscious about it.
Scars – Improved surgical methods mean that most people won’t have major scarring. Surgeons will try to hide scars in skin creases in the neck or on the face, and the scars usually fade over time. Scars from radiation therapy may change the colour or texture of the skin.
Face – In some cases, removing the cancer means removing an eye or part of the jaw, nose, ear or skin. Some people have reconstructive surgery using tissue from another part of the body. Other people may have a prosthesis (e.g. a nose prosthesis), a soft plastic replacement for the tissue that has been removed. A prosthesis will be specially fitted to blend in well with your own features. If you are likely to need a prosthesis, the surgeon will discuss it with you before the operation.
Jaw and teeth – For certain cancers, your surgeon will need to cut through your jaw (mandibulotomy) and reconstruct it with a plate. This involves a cut through your chin and lip, and the scars will be noticeable for some time. If you have lost teeth due to cancer treatment, you may be able to have further surgery to replace or reconstruct them.
Swelling – Surgery or radiation therapy can damage lymph nodes, and cause swelling called lymphoedema.
Tips for adjusting to appearance changes
- Talk about how you are feeling with a family member, friend, social worker, occupational therapist or psychologist.
- Ask your treatment team how surgery will affect your appearance and if you will be offered reconstructive surgery or a prosthesis to rebuild parts of your face and neck. Your team can suggest ways to help you cope and refer you to support services.
- Give yourself time to get used to any changes. Some may be temporary or improve with time.
- Try to see yourself as a whole person (body, mind and personality) rather than focusing only on the part of you that has changed.
- Look Good Feel Better workshops show how to use hats, scarves, make-up and skin care to help boost your self-esteem. Find out more and book at lgfb.org.au.
Sex and intimacy
Head and neck cancer can affect your sex life in emotional and physical ways. Less interest in sex (low libido) is common. Continuing to feel tired after treatment and feeling anxious about cancer returning may also affect your sexual wellbeing. If your appearance has changed, you may grieve for how you used to look or worry about feeling attractive.
Treatment may cause side effects such as dry mouth, bad breath, thick and sticky saliva, poor tongue and lip movement, facial palsy, scars, or a stiff neck and jaw. Mouth surgery may reduce feeling in the tongue or lips, but feeling should return in 12–18 months. These changes can make kissing and oral sex difficult, while any altered speech may affect your self-esteem and ability to express yourself during sex.
During chemotherapy, use barrier contraception (e.g. condoms) during sexual intercourse to avoid exposing your partner to chemotherapy risks and to avoid getting pregnant. It is important to discuss this with your doctor to keep your partner safe and to prevent pregnancy.
You or your partner/s may worry about having sex if the cancer was HPV-related. A long-term partner is likely to have already had the virus and cleared it without having symptoms. Their immune system remembers it and stops an infection developing again. Talk to your doctor about the risk of passing on HPV to a new partner.
Some people choose to express their feelings in ways other than sex, such as cuddling, holding hands or touching cheek-to-cheek. You may wish to talk to a psychologist or sexual health professional, by yourself or with a partner, to help you find ways to adapt to any sexual changes.
Vision changes
If the cancer is in your eye socket, the surgeon may have to remove your eye (orbital exenteration). The empty eye socket will be replaced by a sphere of tissue from another part of your body. This keeps the structure of the eye socket. Later you can be fitted for an artificial eye, painted to look like your other eye and surrounding tissue. The eye is like a large contact lens that fits over the new tissue in the eye socket.
You will still be able to see with your remaining eye, but your depth perception and peripheral vision won’t be as good. The physiotherapist and occupational therapist can assist you to manage any changes to your vision after surgery. You will usually still be able to drive and play sport, but it may take time to get used to the changes. Before you start driving again, tell your driver licensing authority about the changes in your vision, as there may be restrictions you have to follow. The licensing authority may ask for information from your doctor to decide if you are medically fit to drive.
Hearing loss
Ask your treatment team whether you are at risk of hearing loss and if you should have your hearing tested after treatment ends.
Chemotherapy – Some drugs can cause hearing loss. The first sign may be ringing in the ears (tinnitus), so tell your doctors if you notice this.
Radiation therapy – This can damage the internal structure of the ear, cause fluid build-up behind the eardrums and lead to loss of hearing.
Surgery – Some surgeries, especially for nasopharyngeal cancer, can cause temporary or permanent hearing loss.
Lymphoedema
If lymph nodes have been removed in a neck dissection or damaged by radiation therapy, this may prevent lymph fluid from draining properly. The fluid can build up and cause swelling in the neck, face and throat. This is known as lymphoedema. It can be temporary or permanent and may change your appearance. People who have had surgery followed by radiation therapy to the neck are more at risk, especially if both sides of the neck are treated. You are also more likely to develop lymphoedema if a lot of lymph nodes were removed.
Symptoms of lymphoedema can be easier to manage if the condition is treated early. The main signs of lymphoedema include swelling, redness and skin warmth, which may come and go. Sometimes the swelling develops internally and is hard to see but the area may feel different (e.g. mild tingling). It is important to look out for these signs and to visit your doctor if they appear.
Preventing and managing lymphoedema
Sometimes the swelling and other signs of lymphoedema can take months or years to develop, although some people who are at risk never develop the condition.
Some hospitals have specialist physiotherapists and occupational therapists who can teach you simple exercises to reduce your risk of developing lymphoedema, or show you ways to manage it if you have it already. There are also private lymphoedema practitioners who can help with prevention and offer treatments such as lymphatic drainage massage, exercises, low-level laser therapy, skin care and compression garments, if needed. To find a lymphoedema practitioner, visit the Australasian Lymphology Association website.
Key points about managing side effects
Common side effects
- People with a head and neck cancer often experience side effects. Some changes are temporary and go away after treatment. Other changes are permanent and need ongoing management and treatment.
- Common side effects include mouth problems; changes to eating, breathing and speech; swallowing difficulties; and other physical changes.
Mouth and eating problems
- A dry mouth or mouth sores can make it difficult to eat, drink or speak.
- You may experience changes in taste, smell and appetite. These changes are usually temporary, but some people may permanently lose their sense of smell.
- Difficulty swallowing is common and can be managed using exercises, medicines and diet.
- Using a feeding tube may be helpful if you have trouble eating. This may be for a few weeks or it may be long term.
Other physical changes
- Surgery may change the way you look. If you find this distressing or embarrassing, speak to a counsellor or psychologist.
- You may have a tracheostomy or stoma to help you breathe. Support is available.
- You may need therapy after surgery to learn how to speak or communicate in other ways.
- Some people get swelling in the neck or face (lymphoedema). A lymphoedema practitioner can show you ways to manage this.
Sources and references
This edition has been developed by Cancer Council NSW on behalf of all other state and territory Cancer Councils as part of a National Cancer Information Subcommittee initiative.
We thank the reviewers of this booklet: Dr Malinda Itchins, Thoracic Medical Oncologist, Royal North Shore Hospital and Chris O’Brien Lifehouse, NSW; Dr Cynleen Kai, Radiation Oncologist, GenesisCare, VIC; Dr Naveed Alam, Thoracic Surgeon, St Vincent’s Hospital, Epworth Richmond, and Monash Medical Centre, VIC; Helen Benny, Consumer; Dr Rachael Dodd, Senior Research Fellow, The Daffodil Centre, NSW; Kim Greco, Specialist head and neck cancers Nurse Consultant, Flinders Medical Centre, SA; Caitriona Nienaber, 13 11 20 Consultant, Cancer Council WA; Marco Salvador, Consumer; Janene Shelton, xxx Foundation Australia – Specialist head and neck cancers Nurse, Darling Downs Health, QLD; Prof Emily Stone, Respiratory Physician, Department of Thoracic Medicine and xxx Transplantation, St Vincent’s Hospital Sydney, NSW; A/Prof Marianne Weber, Stream Lead, head and neck cancers Policy and Evaluation, The Daffodil Centre, NSW.
We would also like to thank the health professionals, consumers and editorial teams who have worked on previous editions of this title.
References
- National Comprehensive Cancer Network (US), NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Head and Neck Cancers, Version 2.2025.
- J-P Machiels et al., “Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment
and follow-up”, Annals of Oncology, vol. 31, iss. 11, 2020, pp. 1462–75. - P Bossi et al., “Nasopharyngeal carcinoma: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up”, Annals of Oncology, vol. 32, iss. 4, 2020, pp. 452–65.
- C Resteghini et al., “Sinonasal malignancy: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up”, ESMO Open, vol. 10, iss. 2, 2025.
- Australian Institute of Health and Welfare (AIHW), Cancer Data in Australia 2025, AIHW, Canberra, viewed 29 October 2025, aihw.gov.au/reports/cancer/cancer-data-in-australia.

Head and neck cancers
Cancer Council 13 11 20
Call us to talk to a specially trained health professional for free and confidential support and information.
Guide to best cancer care
This head and neck cancers guide explains the standard of high-quality cancer care that all Australians can expect, from diagnosis, to treatment, recovery, and living with cancer.