
Skin cancer
About skin cancer
Find out about the different types of skin cancer and how common they are.


Last updated:
Sources and references 
This page details the 2 most common types of skin cancer – basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). These skin cancers are called non-melanoma skin cancer or keratinocyte cancer. For information about melanoma, see our page about melanoma.
What is skin cancer?
Skin cancer is the uncontrolled growth of abnormal cells in the skin.
Skin cancer types
The 3 main types of skin cancer are:
- basal cell carcinoma (BCC) – about 2 out of 3 skin cancers
- squamous cell carcinoma (SCC) – about 1 in 3 skin cancers
- melanoma – about 1 in 100 skin cancers.
Together, BCC and SCC make up about 99% of skin cancers.
About BCC and SCC - Non-melanoma (keratinocyte) skin cancer
Basal cell carcinoma (BCC) and Squamous cell carcinoma (SCC) are also called non-melanoma skin cancer or keratinocyte cancer.
It is estimated that 1,664 people were diagnosed with non-melanoma skin cancer in 2024.
Basal cell carcinoma (BCC)
BCC accounts for about 70% of non-melanoma skin cancers.
It begins in the lower layer of the epidermis (top, outer layer of the skin). It can appear anywhere on the body but most commonly develops on parts of the body that receive high or intermittent sun exposure (head, face, neck, shoulders and back).
Learn more about the signs and symptoms of BCC.
Squamous cell carcinoma (SCC)
SCC accounts for about 30% of non-melanoma skin cancers.
It begins in the upper layer of the epidermis and usually appears where the skin has had most exposure to the sun (head, neck, hands, forearms and lower legs). SCC generally grows quickly over weeks or months.
Learn more about the signs and symptoms of SCC.
Basal cell carcinoma (BCC) vs. Squamous cell carcinoma (SCC)
| Basal cell carcinoma (BCC) | Squamous cell carcinoma (SCC) | |
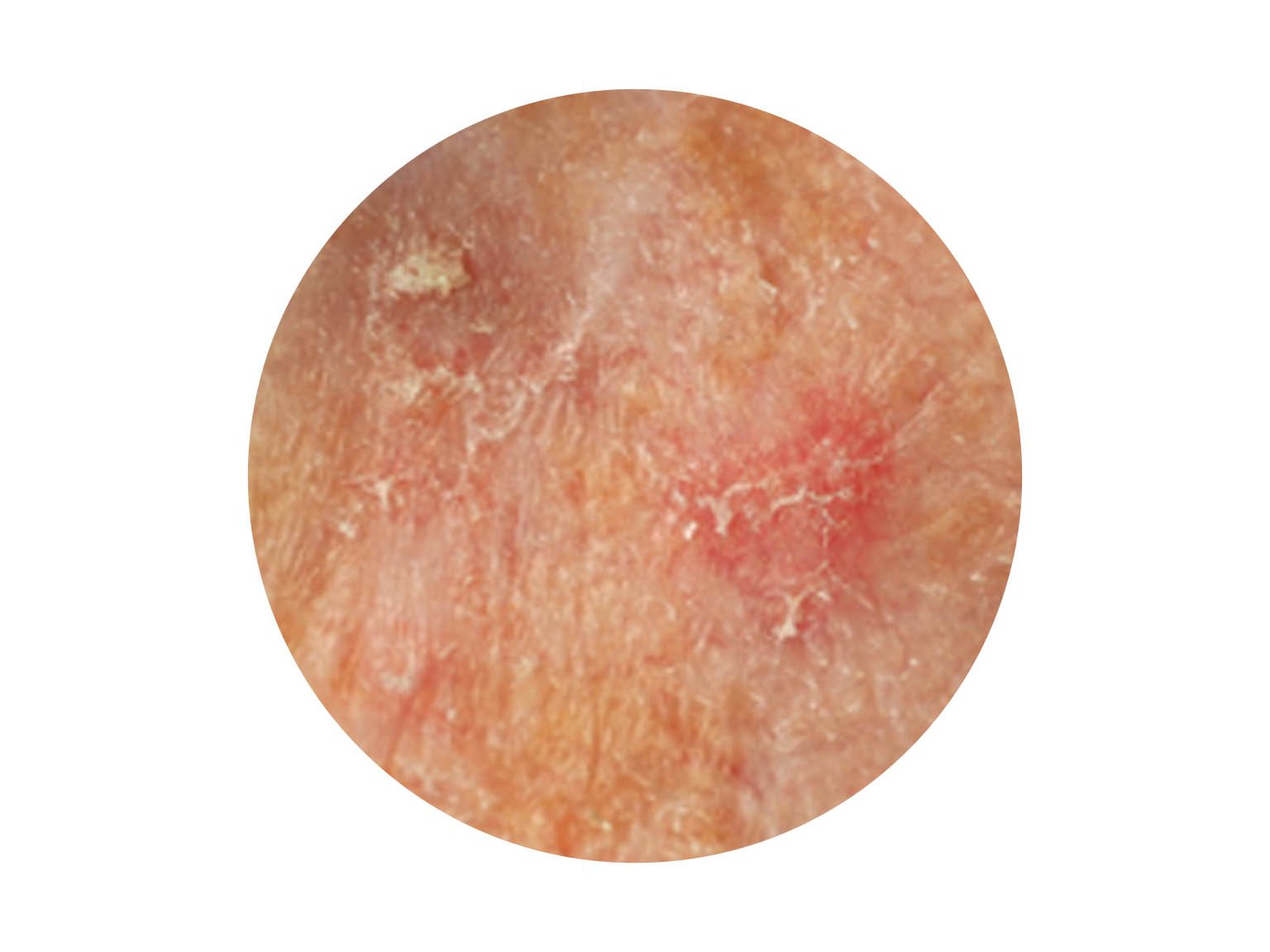
| how it may look |  | 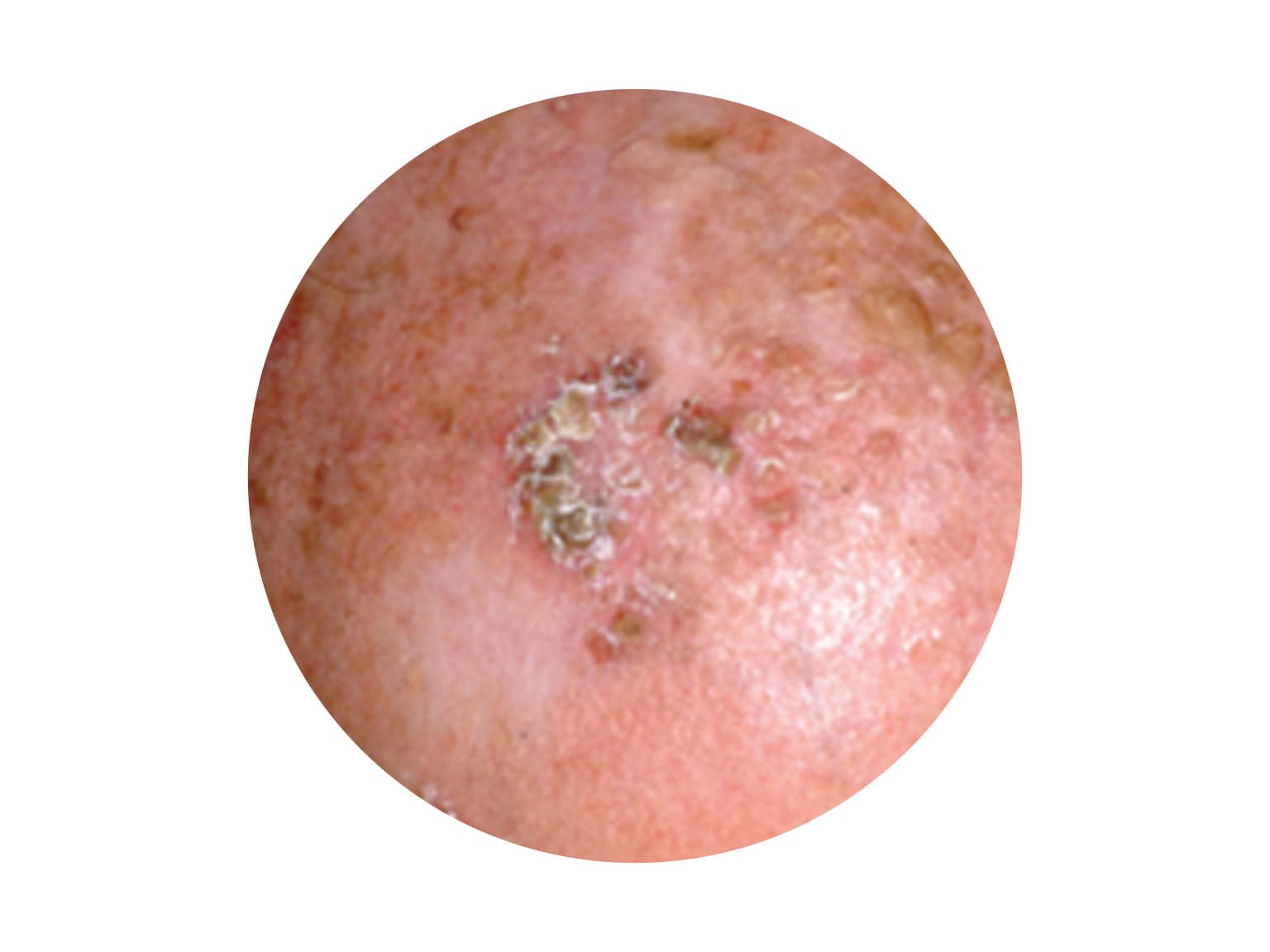 |
| the most common signs | a pink, pearl-like, flat or raised lump; shiny, pale/ bright/dark pink scaly area | a thick scaly lesion; a fast-growing pink lump; a red, scaly or crusted spot |
| what it may feel like | can be itchy, inflamed, ulcerate, weep, ooze, scab or bleed; may “heal” then inflame/bleed/itch again | can become inflamed and often feel tender to the touch; may occasionally bleed |
| where it is most often found | sun-exposed areas, such as head, face, neck, shoulders, arms and legs, but may be anywhere | sun-exposed areas, such as head, face, neck, shoulders, arms and legs, but may be anywhere |
| how it usually grows | slowly over months or years; very rarely spreads to other parts of the body; may grow deeper, invade nerves and tissue, making treatment more difficult | quickly over weeks or months; called invasive SCC if it invades past skin’s top layer; untreated, may spread to other parts of the body (metastatic SCC) |
| the risk factors | having had a BCC increases the risk of developing another BCC | SCCs on head, neck, lips,
|
Non-invasive cancerous lesions
A third group of lesions called keratinocyte dysplasias includes solar keratosis, Bowenoid keratosis and squamous cell carcinoma in-situ (Bowen's disease). These are not invasive cancers, however may require treatment as some may develop into non-melanoma skin cancers.
About melanoma
This starts in the melanocytes and makes up 1–2% of all skin cancers. It is the most serious form of skin cancer because it is more likely to spread to other parts of the body, especially if not found and treated early.
This section is only about non-melanoma (keratinocyte) skin cancers. Visit our melanoma section to read more about melanoma symptoms, diagnosis, and treatment options.
Rare types of skin cancer
These include Merkel cell carcinoma and angiosarcoma. They are treated differently from BCC and SCC. Call Cancer Council 13 11 20 for more information.
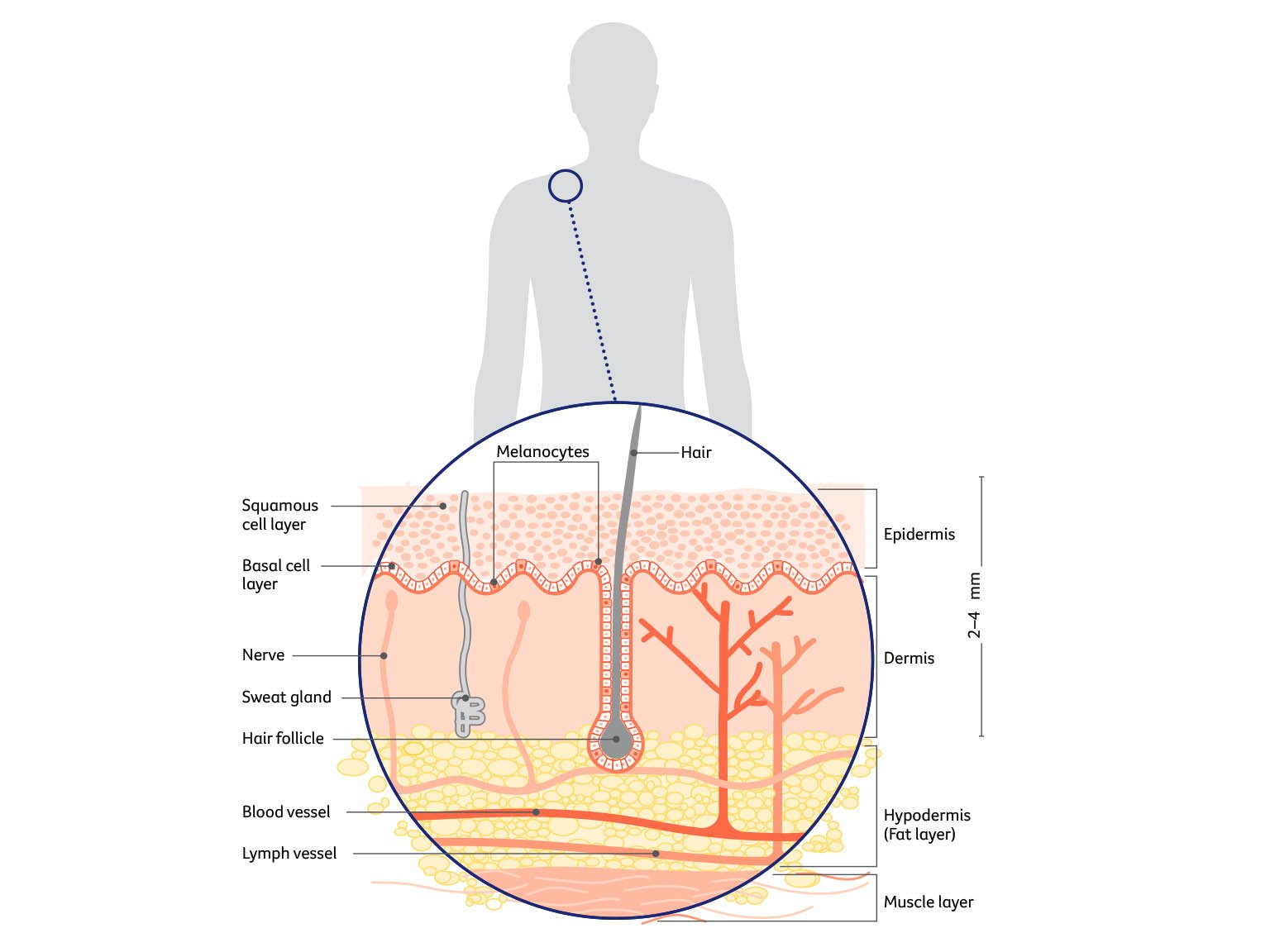
The skin
The skin is the largest organ of the body. It acts as a barrier to protect the body from injury, control body temperature and prevent loss of body fluids. The 2 main layers of the skin are the epidermis and dermis.
Epidermis
This is the top, outer layer of the skin. It has 3 main types of cells:
Squamous cells – These flat squamous cells are packed tightly together to make up the top layer of skin. They form the thickest layer of the epidermis.
Basal cells – These block-like basal cells make up the lower layer of the epidermis. The body makes new basal cells all the time. As they age, they move up into the epidermis and flatten out to form squamous cells.
Both basal and squamous cells are keratinocyte cells, which is why non-melanoma skin cancers are sometimes called keratinocyte cancers.
Melanocytes – These cells sit between the basal cells and produce a dark pigment called melanin that gives skin its colour. When skin is exposed to ultraviolet (UV) radiation, melanocytes make melanin to try to protect the skin from getting burnt. Melanocytes are also found in non-cancerous spots on the skin called moles or naevi.
Dermis
This layer of the skin sits below the epidermis. The dermis is made up of fibrous tissue and contains the roots of hairs (follicles), sweat glands, blood vessels, lymph vessels and nerves.
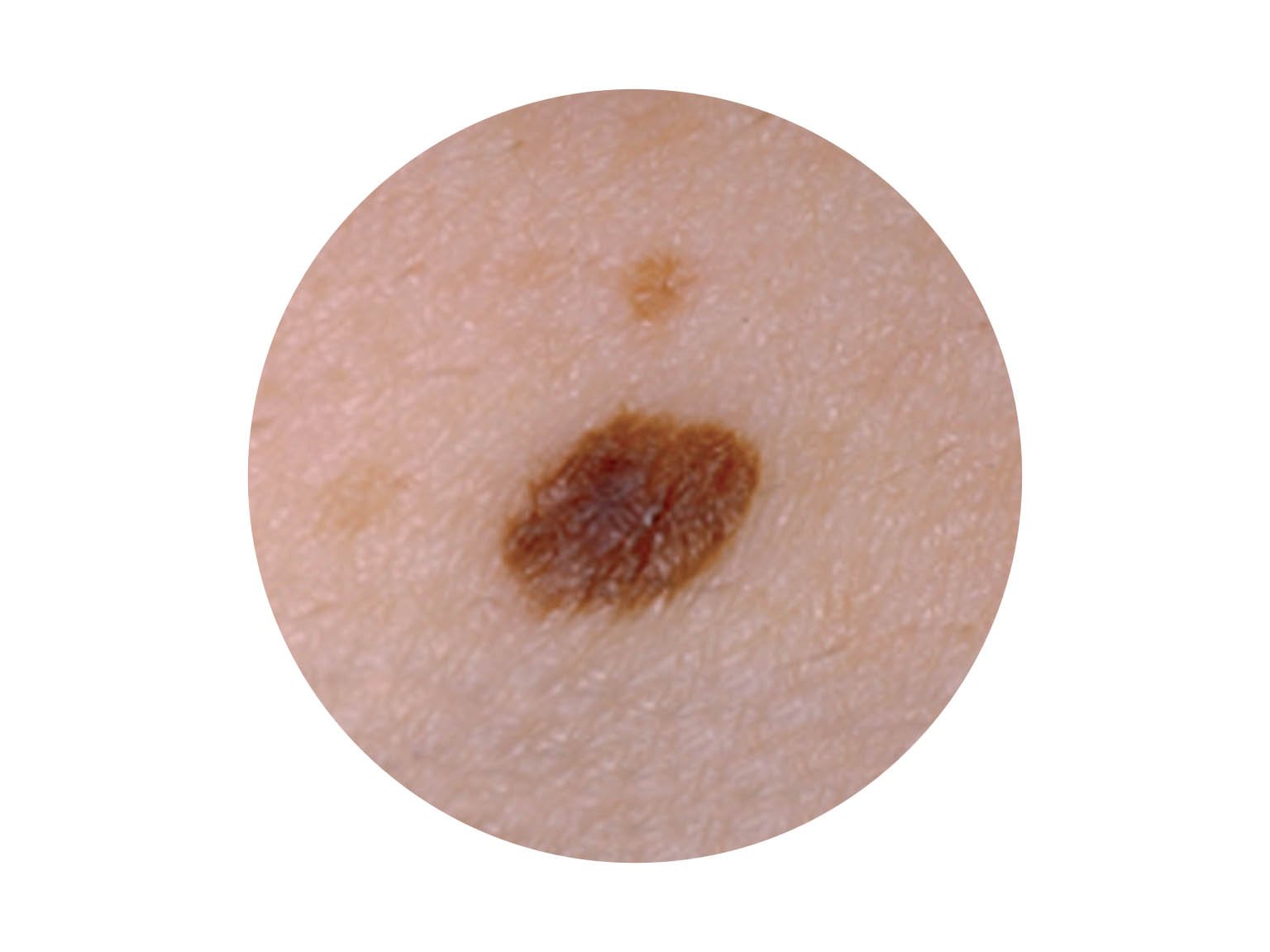
What about other skin spots?
Some spots that appear on the skin are not cancerous. We have given examples of the most common ones here, but these skin spots can vary in how they look. If you are concerned about any mark or growth on your skin, see a general practitioner (GP) or a dermatologist to have it checked.
Types of non-cancerous skin spots
| Sunspot (actinic or solar keratosis) | Age spot (seborrhoeic keratosis) |
 |  |
|
|
GwenI have lots of age spots and moles. I find it hard, but I try to keep track of what they look like, and any changes. But I make sure to get a skin check by a doctor every year too. Last check they found an SCC, but luckily it was treated early."
| Mole (naevus) | Irregular mole (dysplastic naevus) |
 | 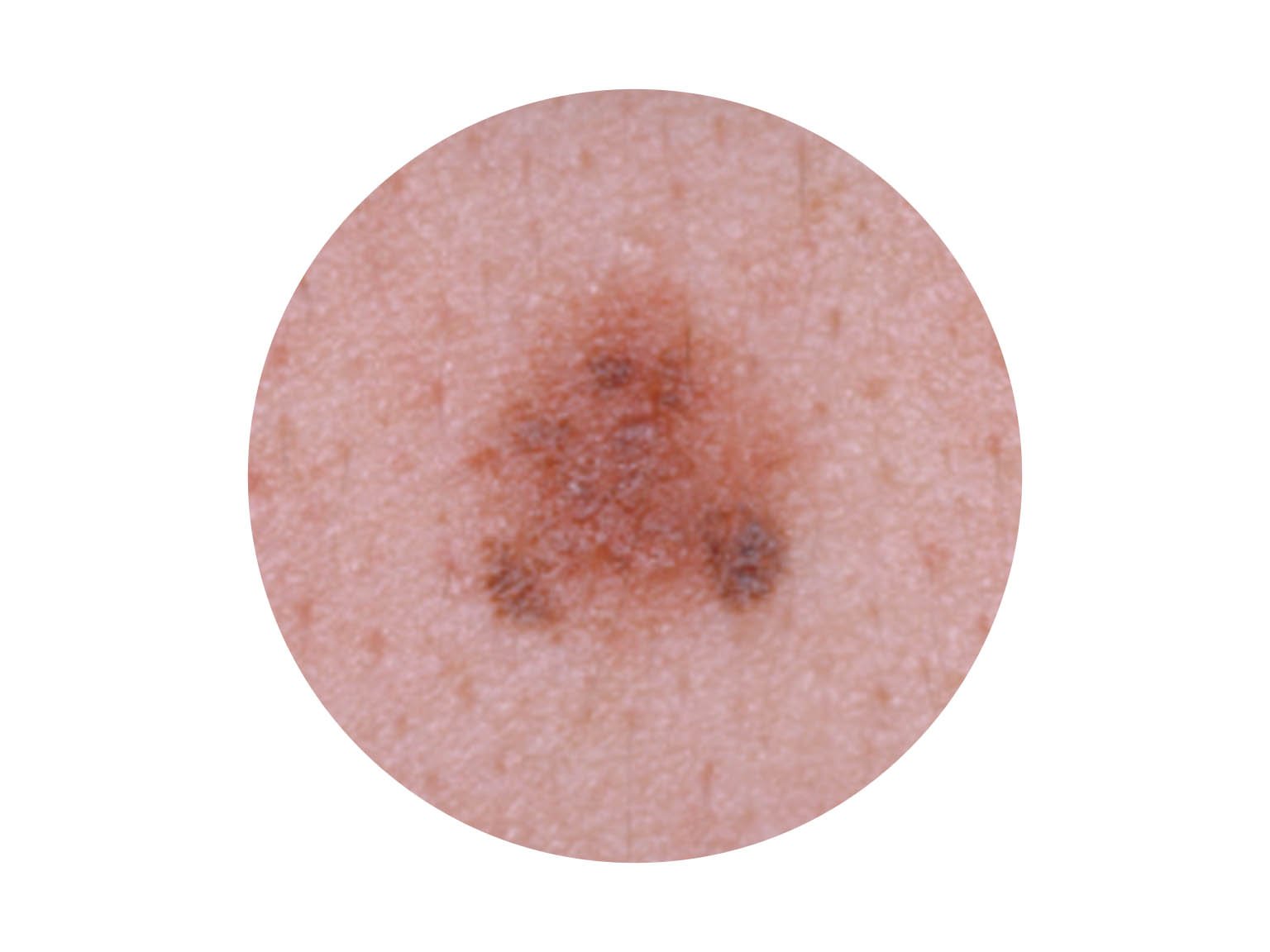 |
|
|
Sources and references
This edition has been developed by Cancer Council NSW on behalf of all other state and territory Cancer Councils as part of a National Cancer Information Subcommittee initiative.
All updated content has been clinically reviewed by Prof Victoria Mar, Director, Victorian Melanoma Service, Alfred Hospital and Monash University, VIC and Prof Anne Cust, Acting Director, The Daffodil Centre, The University of Sydney and Cancer Council NSW, and faculty member, Melanoma Institute Australia.
This edition is based on the previous edition, which was reviewed by the following panel: Prof Victoria Mar (see above); Tracey Bilson, Consumer; Raelene Buchan, Consumer; Alison Button-Sloan, Consumer; Dr Margaret Chua, Radiation Oncologist, and the Skin Radiation Oncology team, Peter MacCallum Cancer Centre, VIC; Prof Anne Cust, (see above); A/Prof Paul Fishburn, Skin Cancer Doctor, Norwest Skin Cancer Centre, NSW and Faculty of Medicine, University of Queensland; Danielle Goss, Melanoma Clinical Nurse Specialist, Amie St Clair Melanoma (part of Melanoma Institute Australia), Wagga Wagga, NSW; Louise Pellerade, 13 11 20 Consultant, Cancer Council WA; Dr Shireen Sidhu, Head of Dermatology, The Royal Adelaide Hospital, SA; Dr Amelia Smit, Research Fellow – Melanoma and Skin Cancer, The Daffodil Centre, The University of Sydney and Cancer Council NSW; Dr Tony Tonks, Plastic and Reconstructive Surgeon, Canberra Plastic Surgery, ACT.
We also thank the health professionals, consumers and editorial teams who have worked on previous editions of this title.
Thanks also to Sydney Melanoma Diagnostic Centre for providing the dysplastic naevus photograph on page 11, A/Prof Paul Fishburn for providing the sunspot photograph on page 10, A/Prof Andrew Miller for providing the age spot photograph on page 10, and Prof H Peter Soyer for providing the other photographs on pages 9–11.

Skin cancer
Cancer Council 13 11 20
Call us to talk to a specially trained health professional for free and confidential support and information.
Guide to best cancer care
This skin cancer guide explains the standard of high-quality cancer care that all Australians can expect, from diagnosis, to treatment, recovery, and living with cancer.