
Head and neck cancers
Radiation therapy for head and neck cancers
Radiation therapy can be given for head and neck cancers as the main treatment, or as treatment after surgery. your oncologist will help you decide if radiation is the right treatment for your cancer type and stage.


Last updated:
Sources and references What's on this page

This treatment (also called radiotherapy) uses a controlled dose of radiation to kill or damage cancer cells. For head and neck cancer, it is most often given with external beam radiation therapy (EBRT). A technique called intensity modulated radiation therapy (IMRT) targets the radiation precisely to the cancer, which reduces treatment time and causes as little harm as possible to nearby healthy tissue.
Radiation therapy as the main treatment – For some pharyngeal and laryngeal cancers, radiation therapy will be the main treatment. The aim is to destroy the cancer while maintaining normal speech, swallowing and breathing. Sometimes chemotherapy will also be used to help the radiation work better (chemoradiation). Radiation treatment usually is given daily for 7 weeks for most head and neck cancers, but this may vary from person to person.
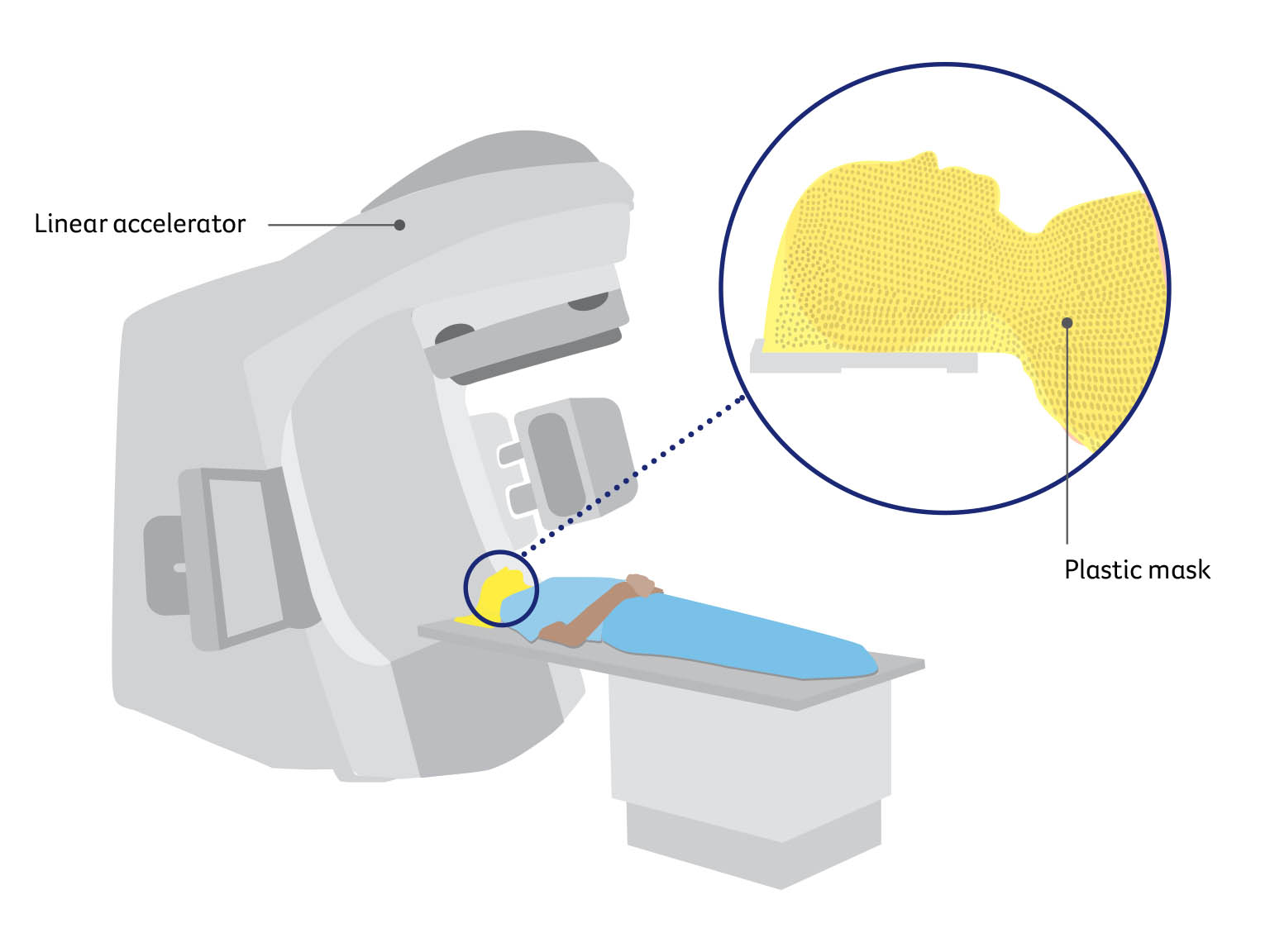
Radiation therapy after surgery – Radiation therapy is often used after surgery for head and neck cancers. This is known as adjuvant treatment. The aim is to destroy any remaining cancer cells and reduce the chance of the cancer coming back. You will probably start radiation therapy as soon as your wounds have healed and you’ve recovered your strength, which should be within 6 weeks. Adjuvant radiation therapy is sometimes given together with chemotherapy (chemoradiation). This is usually given for about 6–7 weeks, but may vary person to person. Before radiation therapy, you meet with a radiation oncologist to work out whether radiation therapy is right for you. You will have a planning session with a CT scan to show the exact area that needs the radiation. You will also be fitted for a plastic mask called an immobilisation mask. You will wear this at each treatment session.
External beam radiation therapy
Having radiation therapy
Radiation therapy is carefully planned to make sure enough radiation reaches the cancer, while as little as possible reaches healthy organs and tissues. During treatment sessions, you will lie on a table under a machine called a linear accelerator, which precisely delivers the radiation. The treatment is painless and is usually given Monday to Friday for 6–7 weeks. You usually won’t need to stay in hospital.
Wearing the mask
You wear the plastic mask for about 10–20 minutes at each session. It helps you keep still and makes sure the radiation is targeted at the same area at each treatment session. You can see and breathe easily, but it may feel strange and confined at first. Tell the radiation therapists if you have claustrophobia or the mask makes you feel uncomfortable – you can talk to someone or may be offered medicine to help you relax.
Side effects of radiation therapy
Radiation therapy side effects vary depending on the area treated, the number of sessions, and whether it is combined with chemotherapy. Side effects often get worse 1–3 weeks after treatment ends and then start to improve. Some side effects may last longer, be ongoing or appear several months or years later. Some may be permanent. It is important to talk to your treatment team if you have any concerns or questions on how the treatment may affect you. The most common short-term and long-term side effects are listed below. For information about managing side effects.
During or immediately after treatment – Short-term side effects can include fatigue, mouth sores, taste changes, nausea, loss of appetite, mouth infection (oral thrush), dry mouth, thick saliva and phlegm, swallowing difficulties, skin redness, burning and pain in the area treated, breathing difficulties and weight loss.
Ongoing – Longer-term or permanent side effects may include dry mouth, thick saliva, difficulties with swallowing and speech, changes in taste, fatigue, muscle stiffness, neck swelling, appetite and weight loss, mouth infection (oral thrush), hoarseness, dental problems such as tooth decay and gum disease, difficulty opening the mouth, and hair loss.
Aspiration – Some people develop a temporary or ongoing problem where fluid or food enters the windpipe (trachea) while swallowing. This is called aspiration and it can cause coughing, lung infections such as pneumonia and, sometimes, difficulty breathing.
Thyroid damage – If the treatment damages the thyroid, it can cause an underactive thyroid (hypothyroidism). This can be managed with thyroid hormone replacement tablets.
Osteoradionecrosis of the jaw – Radiation therapy can damage blood vessels, reducing the blood supply to the area treated. Occasionally, the bone starts to die, leading to pain, infection and fractures. This is known as osteoradionecrosis, or ORN. About 5–7% of people who have radiation therapy to the head and neck develop ORN of the jaw. It can occur months or years later, most commonly after having dental work such as the removal of teeth, when the bone is unable to heal itself. This is why you will usually see a dentist before your cancer treatment, so any dental issues can be treated before there is a risk of ORN.
It is very important to tell your dentist that you have had radiation therapy before beginning any dental work. Treatment for ORN may include antibiotics, other medicines or surgery. To help the bone heal, some people may also have hyperbaric oxygen treatment (breathing in concentrated oxygen in a pressurised chamber).
Treatments for head and neck cancers
Sources and references
This edition has been developed by Cancer Council NSW on behalf of all other state and territory Cancer Councils as part of a National Cancer Information Subcommittee initiative.
We thank the reviewers of this booklet: Dr Malinda Itchins, Thoracic Medical Oncologist, Royal North Shore Hospital and Chris O’Brien Lifehouse, NSW; Dr Cynleen Kai, Radiation Oncologist, GenesisCare, VIC; Dr Naveed Alam, Thoracic Surgeon, St Vincent’s Hospital, Epworth Richmond, and Monash Medical Centre, VIC; Helen Benny, Consumer; Dr Rachael Dodd, Senior Research Fellow, The Daffodil Centre, NSW; Kim Greco, Specialist head and neck cancers Nurse Consultant, Flinders Medical Centre, SA; Caitriona Nienaber, 13 11 20 Consultant, Cancer Council WA; Marco Salvador, Consumer; Janene Shelton, xxx Foundation Australia – Specialist head and neck cancers Nurse, Darling Downs Health, QLD; Prof Emily Stone, Respiratory Physician, Department of Thoracic Medicine and xxx Transplantation, St Vincent’s Hospital Sydney, NSW; A/Prof Marianne Weber, Stream Lead, head and neck cancers Policy and Evaluation, The Daffodil Centre, NSW.
We would also like to thank the health professionals, consumers and editorial teams who have worked on previous editions of this title.
References
- National Comprehensive Cancer Network (US), NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Head and Neck Cancers, Version 2.2025.
- J-P Machiels et al., “Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment
and follow-up”, Annals of Oncology, vol. 31, iss. 11, 2020, pp. 1462–75. - P Bossi et al., “Nasopharyngeal carcinoma: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up”, Annals of Oncology, vol. 32, iss. 4, 2020, pp. 452–65.
- C Resteghini et al., “Sinonasal malignancy: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up”, ESMO Open, vol. 10, iss. 2, 2025.
- Australian Institute of Health and Welfare (AIHW), Cancer Data in Australia 2025, AIHW, Canberra, viewed 29 October 2025, aihw.gov.au/reports/cancer/cancer-data-in-australia.

Head and neck cancers
Cancer Council 13 11 20
Call us to talk to a specially trained health professional for free and confidential support and information.
Guide to best cancer care
This head and neck cancers guide explains the standard of high-quality cancer care that all Australians can expect, from diagnosis, to treatment, recovery, and living with cancer.