
Cervical cancer is the 14th most common cancer affecting Australian women. Australia has one of the lowest rates of cervical cancer incidence and mortality in the world. In 2015 in Australia there were 857 new cases of cervical cancer.[1] In 2016 there were 259 deaths attributable to cervical cancer.[1] The lifetime risk of a woman developing cervical cancer before the age of 85 years is one in 162.
Cervical cancer incidence and mortality rates are three and four times higher respectively for Indigenous women than for non-Indigenous Australian women.[2] Internationally, the large majority of cervical cancer cases (around 85%) and deaths (87%) occur in less developed regions.[5] Incidence rates are lowest in Australia/New Zealand and Western Asia.[5]
In Australia, lower participation in screening and higher rates of cervical cancer incidence and mortality have been reported in women with lower socio-economic disadvantage.[6] Women from culturally and linguistically diverse communities are less likely to participate in cervical screening and are at an increased risk of cervical cancer incidence and mortality.[7][8]
Almost all cases of cervical cancer are attributable to human papillomavirus (HPV) infection. HPV infection is highly prevalent: the estimated lifetime risk for women of one or more genital HPV infections is 80%.[9] It is estimated that around 291 million women worldwide are infected with HPV, almost a third of whom are infected with the high-risk types HPV16 or HPV18 or both,[10] which are present in about 70% of cervical cancers globally. In Australia, the proportion of HPV16/18 positive cervical cancer is higher than global rates at 77%.[11]
The incidence and mortality rates for cervical cancer in Australia both halved after the introduction of the National Cervical Screening Program (NCSP) in 1991 until 2002, and have since remained stable at around nine new cases and two deaths per 100,000 women.[1] Australia’s cervical cancer mortality rate is now among the lowest in the world,[5][12] however this is not consistent for all population groups with mortality rates in Indigenous women similar to less developed regions.[2][5]
The majority of the decline in invasive cervical cancer rates in developed countries is due to a reduction in squamous cell carcinoma. In contrast, the incidence of adenocarcinomas has not declined, largely attributed to difficulties in detecting these types of cancer through cervical screening using the Pap test.[13][14] In Australia the incidence of adenocarcinoma has been increasing since the early to mid-2000s,[15] and this cancer now comprises over one in four of all cervical cancers diagnosed.[6] Trends in age-standardised incidence for different types of cervical carcinomas in Australia are shown in Figure 1.
Figure 1. Incidence of carcinoma of the cervix (squamous cell carcinoma, adenocarcinoma, adenosquamous carcinoma and other and unspecified carcinoma) in women aged 20–69, 1982 to 2013
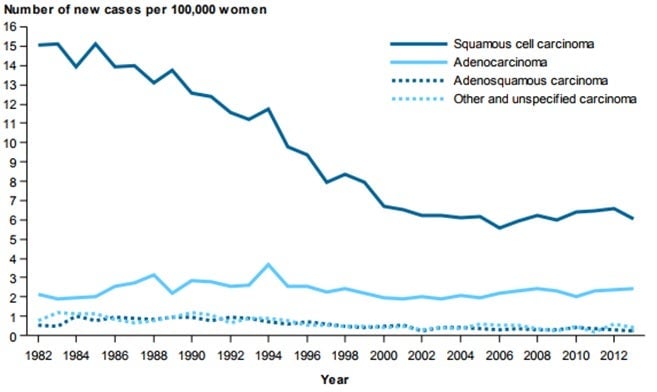
Source: AIHW 2017[16]
Economic impact
The cost of the NCSP in 2017 was estimated at $223 million, excluding overheads.[17] It has been estimated that had the renewed NCSP been in place instead of cytology-based screening, the NCSP would have cost approximately $41 million less in 2017. As the vaccinated cohort matures, the renewed NCSP becomes more favourable in terms of economic impact, as the difference in cost between the previous cytology-based program and the renewed NCSP increases further.
- Australian Institute of Health and Welfare. Australian Cancer Incidence and Mortality (ACIM) books. [homepage on the internet] Canberra: AIHW; 2017 Available from: http://www.aihw.gov.au/acim-books/.
- Australian Institute of Health and Welfare. Cancer in Aboriginal & Torres Strait Islander people of Australia. [homepage on the internet] Canberra: AIHW; 2018 Available from: https://www.aihw.gov.au/reports/cancer/cancer-in-indigenous-australians/contents/cancer-type/cervical-cancer-c53.
- International Agency for Research on Cancer. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. Lyon, France: IARC; 2013 Dec Available from: http://globocan.iarc.fr/.
- Australian Institute of Health and Welfare. Cervical screening in Australia 2018. Canberra: AIHW; 2018. Report No.: Cat. no. CAN 111. Available from: https://www.aihw.gov.au/getmedia/8a26b34d-a912-4f01-b646-dc5d0ca54f03/aihw-can-111.pdf.aspx?inline=true.
- Anaman-Torgbor JA, King J, Correa-Velez I. Barriers and facilitators of cervical cancer screening practices among African immigrant women living in Brisbane, Australia. Eur J Oncol Nurs 2017 Dec;31:22-29 Available from: http://www.ncbi.nlm.nih.gov/pubmed/29173823.
- Aminisani N, Armstrong BK, Egger S, Canfell K. Impact of organised cervical screening on cervical cancer incidence and mortality in migrant women in Australia. BMC Cancer 2012 Oct 23;12:491 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23092207.
- Bekkers RL, Massuger LF, Bulten J, Melchers WJ. Epidemiological and clinical aspects of human papillomavirus detection in the prevention of cervical cancer. Rev Med Virol 2004 Mar;14(2):95-105 Available from: http://www.ncbi.nlm.nih.gov/pubmed/15027002.
- de Sanjosé S, Diaz M, Castellsagué X, Clifford G, Bruni L, Muñoz N, et al. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis. Lancet Infect Dis 2007 Jul;7(7):453-9 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17597569.
- Brotherton JML, Tabrizi SN, Phillips S, Pyman J, Cornall AM, Lambie N, et al. Looking beyond human papillomavirus (HPV) genotype 16 and 18: Defining HPV genotype distribution in cervical cancers in Australia prior to vaccination. Int J Cancer 2017 Oct 15;141(8):1576-1584 Available from: http://www.ncbi.nlm.nih.gov/pubmed/28677147.
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011 Mar;61(2):69-90 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21296855.
- Sasieni P, Castanon A, Cuzick J. Effectiveness of cervical screening with age: population based case-control study of prospectively recorded data. BMJ 2009 Jul 28;339:b2968 Available from: http://www.ncbi.nlm.nih.gov/pubmed/19638651.
- FUTURE I and II Study Group, Ault KA, Joura EA, Kjaer SK, Iversen OE, Wheeler CM, et al. Adenocarcinoma in situ and associated human papillomavirus type distribution observed in two clinical trials of a quadrivalent human papillomavirus vaccine. Int J Cancer 2011 Mar 15;128(6):1344-53 Available from: http://www.ncbi.nlm.nih.gov/pubmed/20949623.
- Smith MA, Canfell K. Projected impact of HPV vaccination and primary HPV screening on cervical adenocarcinoma: Example from Australia. Papillomavirus Res 2017 Jun;3:134-141 Available from: http://www.ncbi.nlm.nih.gov/pubmed/28720447.
- Australian Institute of Health and Welfare. Cervical screening in Australia 2014–2015. Canberra: AIHW; 2017. Report No.: Cancer Series No. 105, Cat. no. CAN 104. Available from: https://www.aihw.gov.au/getmedia/adc621ce-a54a-4680-8b37-2a70d897964a/20434.pdf.aspx?inline=true.
- Lew JB, Simms KT, Smith MA, Hall M, Kang YJ, Xu XM, et al. Primary HPV testing versus cytology-based cervical screening in women in Australia vaccinated for HPV and unvaccinated: effectiveness and economic assessment for the National Cervical Screening Program. Lancet Public Health 2017 Feb;2(2):e96-e107 Available from: http://www.ncbi.nlm.nih.gov/pubmed/29253402.
