

Vitamin D is a hormone which regulates calcium levels in the blood, and has many important consequences for bone and muscle health. Adequate (greater than 50nmol/L) vitamin D is required to develop and maintain healthy bones and muscles, and in the prevention of osteoporosis and osteomalacia.[1] Inadequate vitamin D levels (less than 50nmol/L) may lead to rickets in young children due to calcium deficiency,[2] and in exclusively breastfed infants whose mothers are vitamin D deficient.[3][4]
There have also been links identified between vitamin D deficiency and an increased risk of bowel cancer, heart disease, infections and auto-immune diseases.[1] However, a recent systematic review notes the paucity of intervention studies showing improved outcomes with increased vitamin D levels following vitamin D supplementation, and suggests that low vitamin D may be a by-product, rather than cause, of associated conditions.[5] Another meta-analysis has recently shown that vitamin D supplementation does not reduce the relative risk of heart attack, stroke, cancer, or bone fractures (total and hip fractures) in the general population by 15% or more. However, vitamin D appeared to reduce the risk of hip fractures among people in residential care with more efficacy, when combined together with calcium supplementation.[6] Yet another meta-analysis concluded that there is "no clear role for vitamin D" for any of the outcomes examined in the observational and/or randomised controlled trials conducted thus far.[7] Mortality outcomes have also been examined and related to circulating vitamin D or vitamin D supplementation in recent meta-analyses.[6][8] A 2019 meta-analysis concluded that vitamin D supplementation was not associated with all cause mortality, cardiovascular mortality, or non-cancer, non-cardiovascular mortality in adults. However, vitamin D supplementation was associated with a reduced risk of cancer mortality by 16%.[9] This is an ongoing area of research and further studies and better design trials are needed to draw firm, universal conclusions.
The Australian Bureau of Statistics estimates that one in four Australian adults are vitamin D deficient (<50nmol/L), with 7% having a moderate or severe deficiency (<29 nmol/L).[10]
Exposure to UVB radiation (280-315 nm) is the main source of vitamin D.[1] Vitamin D is made through a series of biochemical processes that start when the skin is exposed to UV radiation.[1] There are also dietary sources of vitamin D; in Australia all oil spreads (i.e. low-fat spreads and table margarine) are fortified with vitamin D, as well as some milk and milk products (yoghurts, cheeses etc). Fatty fish, such as salmon, are also a source of vitamin D.[11] However, dietary sources of vitamin D are unlikely to contribute more than 5-10% of an adult’s vitamin D intake in Australia.[11]
Sun exposure and vitamin D
The amount of sunlight required for adequate vitamin D levels depends on a range of factors including UV level (and therefore season), length of exposure and an individual’s skin type. UV levels vary across Australia and throughout the year, as shown in Table 1.
Table 1: Australian capital city average daily maximum UV levels by month.[12]
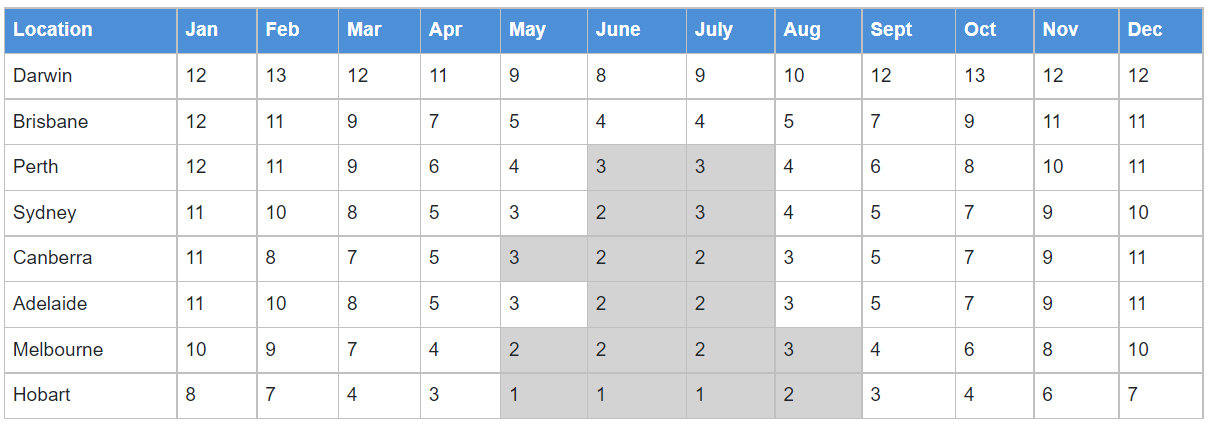
Values are rounded to the nearest whole number. Highlighted months have an average daily maximum UV Index less than 3, even where rounding has made it appear otherwise.
In 2016, Cancer Council Australia, along with the Australasian College of Dermatologists, the Australian and New Zealand Bone and Mineral Society, Osteoporosis Australia and the Endocrine Society of Australia released a set of guidelines to ensure consistency of public health advice relating to UV, vitamin D and sun protection.[13] The guidelines reinforce the importance of sun protection when UV levels are 3 or above, and provide advice regarding the times of day and year in which it is safer to go outside without sun protection. This varies, depending on latitude and season.
During summer in Australia, all states experience periods during the day when UV levels reach three or above (Table 1). In summer, most Australian adults will maintain adequate vitamin D levels during typical day-to-day outdoor activities (see Vitamin D deficiency, below). Whenever the UV level reaches 3 or above, a combination of sun protection measures is recommended when outdoors for more than a few minutes to reduce the risk of skin cancer.
In winter in the southern parts of Australia, where UV radiation levels are below three all day, sun protection is not recommended. At this time of year, people are encouraged to be outdoors around midday each day, with some skin uncovered. The exception to this is outdoor workers, who are unlikely to be deficient in Vitamin D given the long periods of time they spend outdoors, but have an increased risk of skin cancer.[14] For these reasons, Cancer Council recommends that outdoor workers or those working near highly reflective surfaces use sun protection year round, even when the UV Index is below 3.[15]
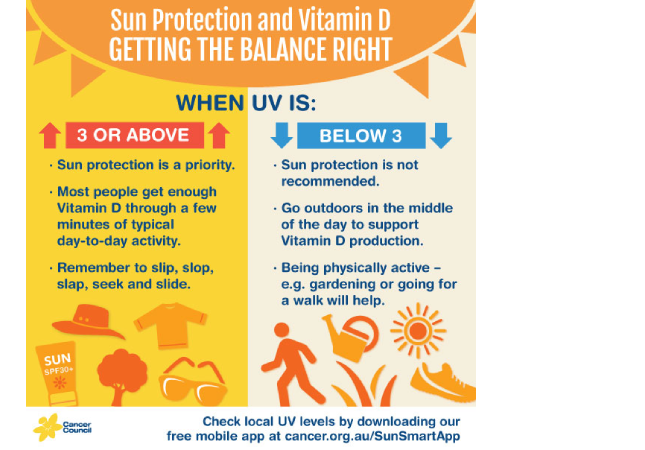
Figure 2: How to use the UV level to balance sun protection and vitamin D.
Prolonged sun exposure does not result in increased vitamin D levels (as excess vitamin D is broken down into inactive metabolites[16]), but does increase the risk of skin cancer.[17] Short periods of sun exposure may be more efficient at producing vitamin D.[18] Daily exercise also assists the body to produce vitamin D.[19]
The AusD Study reported that modifiable behavioral factors strongly influence serum 25(OH)D concentrations in Australian adults. In particular, the findings indicate that reducing clothing cover and increasing the amount of skin exposed is a more effective way to increase vitamin D levels than increasing the time spent outdoors.[20] In winter, people spend less time outside with their skin exposed, which contributes to seasonal decreases in vitamin D levels.[21]
People with naturally very dark skin may need more sun exposure than those with fair to olive skin to achieve the same levels of vitamin D, as the melanin in dark skin affects UV penetration.[22][23] All skin types can be damaged by too much UV radiation.
Individuals at risk of deficiency
- People with naturally very dark skin.[22][23] The pigment in skin (melanin) acts as a filter to UVB radiation and reduces synthesis of vitamin D.
- People with little or no sun exposure.[1] This group includes:
- Older adults - especially the frail - who are in medium to long-term residential care, aged care or housebound, where it can be difficult to get enough sun exposure.
- People who wear concealing clothing for religious or cultural purposes, which may not allow exposure of adequate skin.
- People who deliberately avoid sun exposure for cosmetic or health reasons.
- People at high risk of skin cancers and who therefore avoid exposure to the sun.
- People who spend long hours indoors, including those hospitalised long-term, and those whose mobility is impaired.
- People in occupations where they have limited incidental UV exposure throughout the day, such as taxi drivers, factory workers, night-shift workers.
- Breast-fed babies of mothers who fall into the risk categories above or have mothers with low vitamin D.[24] Breast milk contains little vitamin D and infants initially depend on maternal stores (formula milk is fortified with vitamin D).
- People with conditions (obesity, end-stage liver disease, renal disease and fat malabsorption syndromes such as cystic fibrosis, coeliac disease, inflammatory bowel disease) or taking medications affecting vitamin D metabolism.[25]
Low levels of vitamin D may have no obvious symptoms, but without treatment can have significant health effects.[26] Individuals concerned about vitamin D levels should consult their GP.
Optimal blood vitamin D concentration
Based on current evidence, there is general consensus that a vitamin D level of 50-60 nmol/L (20ng/mL) is sufficient to maintain bone health.[1][27] Given the potential for seasonal decreases in vitamin D, it is recommended that vitamin D levels are 60-70 nmol/L at the end of summer or >50 nmol/L at the end of winter.[1]
An international panel of experts has recommended 25-OH-D levels of >75nmol/L for "individuals with or at risk for musculoskeletal health problems, cardiovascular disease, autoimmune disease and cancer".[28] However, there is insufficient evidence to support this recommendation for the general population.[1]
There are large interpersonal variations as to how much vitamin D will be made for a given dose of UVB. Some of the contributing factors include skin type[22], age (about 50% less vitamin D will be synthesised by an 80-year-old compared with a 20-year-old)[29], obesity (as vitamin D is stored in fat tissue)[30] and baseline vitamin D status (in response to a given dose of UVB, vitamin D levels increase more when the baseline levels are low, than when baseline levels are high).[31]
Vitamin D deficiency in Australia
The Australian Bureau of Statistics estimates that just under one in four (23%) Australian adults are vitamin D deficient (<50nmol/L); 17% are mildly deficient (30-49 nmol/L), 6% are moderately deficient (13-29 nmol/L) and 1% are severely deficient (<13nmol/L).[10] The Australian Health Survey showed that in 2011-12 vitamin D deficiency ranged from 31% in those aged 18–34 years to 15% in those aged 65–74 - it should be noted that vitamin D supplements were more commonly used among older people.[10]
Rates of deficiency were shown to be lower in summer (14%) and higher in winter (36%). There was little variation between the states and territories in summer, when deficiency levels were low across the country; ranging from 6% in Queensland to 19% in New South Wales. A divide was apparent in winter, with rates of vitamin D deficiency particularly high for those living in Victoria and ACT, where nearly one in every two people (49%) were vitamin D deficient in winter, compared with only 16% and 13% respectively in summer. In comparison, vitamin D deficiency remained relatively low in winter for those in Queensland and the Northern Territory.[10] Differences were also seen across each state or territory - vitamin D deficiency was more common among those living in major cities (27%) compared with those living in inner regional (16%), outer regional (13%) and remote areas (9%).[10]
Country of birth was also shown to have an association with vitamin D, with deficiency more common among those born in Southern and Central Asia (67%) as well as North East Asia (64%), South East Asia (58%) and North Africa and the Middle East (50%). This was despite the fact that those born in Southern and Central Asia, North Africa and the Middle East had relatively high rates of vitamin D supplement use (14% and 15% respectively compared with 4% of those born in Australia).[10] Rates of deficiency also remained very high during summer, with 60% of people who were born in Southern and Central Asia and 50% of people who were born in South East Asia still being deficient in December to February.
A person's vitamin D level was also found to be associated with the type of work that they do. Those employed in occupations that were mostly based inside, such as sales workers (28%) and professionals (26%), were more likely to have a vitamin D deficiency than those working in jobs based mostly outdoors, such as machinery operators and drivers (18%).[10] However, these vocational differences were much less pronounced during the summer months. These occupational findings align with two studies conducted in Queensland showing that, even in a subtropical climate, vitamin D insufficiency was prevalent among indoor workers (30[32] -51% in winter and 14% in summer[33]).
Testing vitamin D
Vitamin D testing is recommended for those at risk of vitamin D deficiency; routine screening of healthy adults (including pregnant women), children and infants is not recommended by the Royal College of Pathologists of Australia.[34] Over-testing for vitamin D in Australia became evident after an analysis of 2006-2010 Medicare data found there were 4.5 million tests performed and a 94-fold increase in testing from 2000 to 2010.[35] To address this increase in testing, the Medicare Benefits Schedule was changed in November 2014 to restrict the Medicare rebate to patients who are considered to be at risk of vitamin D deficiency (see MBS online for patient criteria for vitamin D testing).
The best indicator of vitamin D status, and the measure recommended by the Royal College of Pathologists of Australia, is 25-hydroxyvitamin D (25OH-D),[34][36] which may be assessed by automated commercial immunoassay or Liquid chromatographic separation followed by tandem mass spectrometric detection (LC-MS/MS). A systematic review by Wallace and colleagues concluded that these methods have comparable sensitivity for detecting severe vitamin D deficiency (<25 nmol/L).[37]
In most Australian laboratories, automated immunoassay is used for vitamin D testing.[34] The Royal College of Pathologists of Australia warns clinicians to be aware of the limitations of vitamin D testing and recommends that follow-up vitamin D testing be conducted in the same laboratory.[34]
The method that currently has highest sensitivity and specificity is LC-MS/MS. However this method is high-cost, suffers from interference from other metabolites, and potential calibration issues and differences in sample preparation can lead to variable results.[34] All tests should have independent auditing of results regardless of testing method. The international Vitamin D Standardization Program (VSDP) is aiming to standardise the measurement of vitamin D across all laboratories to enable the transfer of findings to patient care and public health activities.[38]
Last modified: 27 July 2020
- Nowson CA, McGrath JJ, Ebeling PR, Haikerwal A, Daly RM, Sanders KM, et al. Vitamin D and health in adults in Australia and New Zealand: a position statement. Med J Aust 2012 Jun 18;196(11):686-7 Available from: http://www.ncbi.nlm.nih.gov/pubmed/22708765.
- Wagner CL, Greer FR, American Academy of Pediatrics Section on Breastfeeding, American Academy of Pediatrics Committee on Nutrition. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics 2008 Nov;122(5):1142-52 Available from: http://www.ncbi.nlm.nih.gov/pubmed/18977996.
- Thomson K, Morley R, Grover SR, Zacharin MR. Postnatal evaluation of vitamin D and bone health in women who were vitamin D-deficient in pregnancy, and in their infants. Med J Aust 2004 Nov 1;181(9):486-8 Available from: http://www.ncbi.nlm.nih.gov/pubmed/15516192.
- Nozza JM, Rodda CP. Vitamin D deficiency in mothers of infants with rickets. Med J Aust 2001 Sep 3;175(5):253-5 Available from: http://www.ncbi.nlm.nih.gov/pubmed/11587256.
- Autier P, Boniol M, Pizot C, Mullie P. Vitamin D status and ill health: a systematic review. Lancet Diabetes Endocrinol 2014 Jan;2(1):76-89 Available from: http://www.ncbi.nlm.nih.gov/pubmed/24622671.
- Bolland MJ, Grey A, Gamble GD, Reid IR. The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: a trial sequential meta-analysis. Lancet Diabetes Endocrinol 2014 Apr;2(4):307-20 Available from: http://www.ncbi.nlm.nih.gov/pubmed/24703049.
- Theodoratou E, Tzoulaki I, Zgaga L, Ioannidis JP. Vitamin D and multiple health outcomes: umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials. BMJ 2014 Apr 1;348:g2035 Available from: http://www.ncbi.nlm.nih.gov/pubmed/24690624.
- Chowdhury R, Kunutsor S, Vitezova A, Oliver-Williams C, Chowdhury S, Kiefte-de-Jong JC, et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ 2014 Apr 1;348:g1903 Available from: http://www.ncbi.nlm.nih.gov/pubmed/24690623.
- Zhang Y, Fang F, Tang J, Jia L, Feng Y, Xu P, et al. Association between vitamin D supplementation and mortality: systematic review and meta-analysis. BMJ 2019 Aug 12;366:l4673 Available from: http://www.ncbi.nlm.nih.gov/pubmed/31405892.
- Australian Bureau of Statistics. 4364.0.55.006 - Australian Health Survey: Biomedical Results for Nutrients, Vitamin D 2011-12. Canberra, Australia: Australian Bureau of Statistics; 2014 Available from: http://www.abs.gov.au/ausstats/abs@.nsf/latestProducts/4364.0.55.006Media%20Release22011-12.
- Nowson CA, Margerison C. Vitamin D intake and vitamin D status of Australians. Med J Aust 2002 Aug 5;177(3):149-52 Available from: http://www.ncbi.nlm.nih.gov/pubmed/12149085.
- Gies P. Capital city maximum UV levels by month. Melbourne, Australia: Australian Radiation Protection and Nuclear Safety Agency; 2013.
- Australian and New Zealand Bone and Mineral Society, the Australasian College of Dermatologists, Cancer Council Australia, Endocrine Society of Australia and Osteoporosis Australia. Position statement - Sun exposure and vitamin D - risks and benefits. [homepage on the internet] Cancer Council Australia; 2016 Jan [cited 2016 Feb 9; updated 2016 Jan]. Available from: http://wiki.cancer.org.au/policy/Position_statement_-_Risks_and_benefits_of_sun_exposure.
- Fritschi L, Driscoll T. Cancer due to occupation in Australia. Aust N Z J Public Health 2006 Jun;30(3):213-9 Available from: http://www.ncbi.nlm.nih.gov/pubmed/16800196.
- Cancer Council. Skin cancer and outdoor work: A work health and safety guide. Cancer Council; 2018.
- Gilchrest BA. Sun exposure and vitamin D sufficiency. Am J Clin Nutr 2008 Aug;88(2):570S-577S Available from: http://www.ncbi.nlm.nih.gov/pubmed/18689404.
- van der Pols JC, Russell A, Bauer U, Neale RE, Kimlin MG, Green AC. Vitamin D status and skin cancer risk independent of time outdoors: 11-year prospective study in an Australian community. J Invest Dermatol 2013 Mar;133(3):637-41 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23076499.
- Norman AW. Sunlight, season, skin pigmentation, vitamin D, and 25-hydroxyvitamin D: integral components of the vitamin D endocrine system. Am J Clin Nutr 1998 Jun;67(6):1108-10 Available from: http://www.ncbi.nlm.nih.gov/pubmed/9625080.
- Scragg R, Holdaway I, Jackson R, Lim T. Plasma 25-hydroxyvitamin D3 and its relation to physical activity and other heart disease risk factors in the general population. Ann Epidemiol 1992 Sep;2(5):697-703 Available from: http://www.ncbi.nlm.nih.gov/pubmed/1342321.
- Kimlin MG, Lucas RM, Harrison SL, van der Mei I, Armstrong BK, Whiteman DC, et al. The contributions of solar ultraviolet radiation exposure and other determinants to serum 25-hydroxyvitamin D concentrations in Australian adults: the AusD Study. Am J Epidemiol 2014 Apr 1;179(7):864-74 Available from: http://www.ncbi.nlm.nih.gov/pubmed/24573539.
- Kimlin M, Sun J, Sinclair C, Heward S, Hill J, Dunstone K, et al. Are the current Australian sun exposure guidelines effective in maintaining adequate levels of 25-hydroxyvitamin D? J Steroid Biochem Mol Biol 2015 Mar 20 Available from: http://www.ncbi.nlm.nih.gov/pubmed/25797374.
- Clemens TL, Adams JS, Henderson SL, Holick MF. Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. Lancet 1982 Jan 9;1(8263):74-6 Available from: http://www.ncbi.nlm.nih.gov/pubmed/6119494.
- Armas LA, Dowell S, Akhter M, Duthuluru S, Huerter C, Hollis BW, et al. Ultraviolet-B radiation increases serum 25-hydroxyvitamin D levels: the effect of UVB dose and skin color. J Am Acad Dermatol 2007 Oct;57(4):588-93 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17637484.
- Munns CF, Simm PJ, Rodda CP, Garnett SP, Zacharin MR, Ward LM, et al. Incidence of vitamin D deficiency rickets among Australian children: an Australian Paediatric Surveillance Unit study. Med J Aust 2012 Apr 16;196(7):466-8 Available from: http://www.ncbi.nlm.nih.gov/pubmed/22509879.
- Royal College of Pathologists of Australia. Position statement: Use and Interpretation of Vitamin D testing. Surry Hills, Australia: Royal College of Pathologists of Australia; 2013.
- Joshi D, Center JR, Eisman JA. Vitamin D deficiency in adults. Australian Prescriber 2010 Jan 1;33(4):103-6.
- Institute of Medicine. Dietary reference intakes for calcium and vitamin D. Washington, United States of America: The National Academies Press; 2011 Available from: http://www.nap.edu/catalog/13050.html.
- Souberbielle JC, Body JJ, Lappe JM, Plebani M, Shoenfeld Y, Wang TJ, et al. Vitamin D and musculoskeletal health, cardiovascular disease, autoimmunity and cancer: Recommendations for clinical practice. Autoimmun Rev 2010 Sep;9(11):709-15 Available from: http://www.ncbi.nlm.nih.gov/pubmed/20601202.
- MacLaughlin J, Holick MF. Aging decreases the capacity of human skin to produce vitamin D3. J Clin Invest 1985 Oct;76(4):1536-8 Available from: http://www.ncbi.nlm.nih.gov/pubmed/2997282.
- Blum M, Dolnikowski G, Seyoum E, Harris SS, Booth SL, Peterson J, et al. Vitamin D(3) in fat tissue. Endocrine 2008 Feb;33(1):90-4 Available from: http://www.ncbi.nlm.nih.gov/pubmed/18338271.
- Bogh MK, Schmedes AV, Philipsen PA, Thieden E, Wulf HC. Vitamin D production after UVB exposure depends on baseline vitamin D and total cholesterol but not on skin pigmentation. J Invest Dermatol 2010 Feb;130(2):546-53 Available from: http://www.ncbi.nlm.nih.gov/pubmed/19812604.
- Jayaratne N, Russell A, van der Pols JC. Sun protection and vitamin D status in an Australian subtropical community. Prev Med 2012 Aug;55(2):146-50 Available from: http://www.ncbi.nlm.nih.gov/pubmed/22634425.
- Vu LH, Whiteman DC, van der Pols JC, Kimlin MG, Neale RE. Serum vitamin D levels in office workers in a subtropical climate. Photochem Photobiol 2011 May;87(3):714-20 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21255019.
- The Royal College of Pathologists Australia. Position statement: Use and interpretation of vitamin D testing. Surry Hills, Australia: The Royal College of Pathologists Australia; 2019 [cited 2020 Jul 16] Available from: https://www.rcpa.edu.au/Library/College-Policies.
- Bilinski K, Boyages S. Evidence of overtesting for vitamin D in Australia: an analysis of 4.5 years of Medicare Benefits Schedule (MBS) data. BMJ Open 2013 Jun 20;3(6) Available from: http://www.ncbi.nlm.nih.gov/pubmed/23794593.
- Seamans KM, Cashman KD. Existing and potentially novel functional markers of vitamin D status: a systematic review. Am J Clin Nutr 2009 Jun;89(6):1997S-2008S Available from: http://www.ncbi.nlm.nih.gov/pubmed/19403634.
- Wallace AM, Gibson S, de la Hunty A, Lamberg-Allardt C, Ashwell M. Measurement of 25-hydroxyvitamin D in the clinical laboratory: current procedures, performance characteristics and limitations. Steroids 2010 Jul;75(7):477-88 Available from: http://www.ncbi.nlm.nih.gov/pubmed/20188118.
- National Institutes of Health Office of Dietary Supplements. Vitamin D Standardization Program Symposium: Tools to Improve Laboratory Measurement. National Institutes of Health; 2013 Available from: http://ods.od.nih.gov/Research/vdsp.aspx.